What is the evidence for opioid analgesia for low back pain?

Back pain
Pain
Opioid analgesics are commonly prescribed to treat low back pain. There is currently no evidence to support prescribing these medicines for people with acute low back pain, and only small pain relief is gained from opioid analgesics in people with chronic low back pain. Furthermore, concern is growing over adverse events and prescription opioid overdose and death.
- Low back pain clinical practice guidelines do not endorse the routine use of opioid analgesics.
- Management of patients with acute and chronic low back pain should begin with reassurance and advice, including recommendation of appropriate nonpharmacological interventions.
- If nonpharmacological pain relief is insufficient for patients with acute low back pain, then use pharmacotherapy such as NSAIDs.
- If nonpharmacological pain relief is insufficient for patients with chronic low back pain, then pharmacological treatments such as NSAIDs or weak opioid analgesics (if the benefits outweigh the risks) may be considered.
- For patients who have been on long-term opioid therapy and have had an inadequate response, consider opioid dose tapering and cessation.
- There is moderate-quality evidence of a small benefit from opioid analgesics in managing chronic low back pain in the short term (less than three months after commencing).
Picture credit: © Sebra/stock.adobe.com
Low back pain, defined as pain between the 12th rib and buttock crease, affects more than 80% of individuals during their lifetime.1 It is the leading cause of disability in Australasia and a common condition keeping Australians out of the workforce, reducing gross domestic product by $3.2 billion per annum.2,3
Pharmacological treatment of acute and chronic low back pain poses challenges for doctors. In this article, we discuss the benefits, risks and challenges associated with pharmacological therapy for low back pain, focusing on treatment with opioid analgesics.
Pharmacological management
The management of low back pain can be a clinical challenge. Practice guidelines traditionally have suggested a stepwise approach to pharmacological treatment, beginning with simple analgesics such as paracetamol or NSAIDs. However, a key challenge now is recommending appropriate pharmacotherapy amid the growing evidence that simple analgesics, such as paracetamol and NSAIDs, offer no or modest benefit for this condition.
A recent review of paracetamol for acute low back pain showed that paracetamol was no more effective than placebo, and carried about a fourfold greater risk of abnormal liver function test results (risk ratio, 3.8; 95% confidence interval [CI], 1.9 to 7.4).7 Furthermore, although a meta-analysis has shown that NSAIDs have a small benefit for acute low back pain (reduction of pain of 6.4 points on a 100-point pain scale; 95% CI, −10.3 to −2.5), gastrointestinal, renal and cardiovascular adverse events are common with these medicines, especially during regular use and in those with risk factors such as pre-existing cardiovascular disorders.8 This study also found that people treated with NSAIDs for spinal pain were 2.5 times more likely to experience gastrointestinal adverse events than people taking a placebo.8 The most recent clinical practice guidelines in the UK and USA recommend that paracetamol should not be offered alone for the treatment of acute low back pain and that NSAIDs should be used at the lowest effective dose.9,10
Increasing use of opioid analgesics
Interestingly, despite widespread use of opioid analgesics for low back pain, the guidelines also do not recommend their use for this condition.9-14 This is because there is limited evidence for their efficacy and a well-established profile of medicine- related harmful effects.15
In Australia, opioid analgesics and opioid analgesic combination medicines are among the most commonly prescribed pharmacological treatments for back pain. This includes the paracetamol and codeine combination and oxycodone.11,12 Furthermore, the most recent analysis of opioid prescribing patterns in Australia showed that 45.6% of all analgesic medicines recommended for acute and chronic spinal (back and neck) pain in 2013/2014 were opioid analgesics.13 However, treatment of low back pain using opioid analgesics is the subject of considerable debate, particularly as there is currently no evidence to guide the use of these medicines in patients with acute low back pain.
Concerns and lack of evidence
Most of the evidence surrounding opioid analgesic use for low back pain comes from trials evaluating use in patients with chronic low back pain. A systematic review published in 2016 found that opioid analgesics provided a small amount of pain relief (reduction of 10.1 points on a 100-point pain scale; 95% CI, −12.8 to −7.4) for patients with chronic low back pain in the short term (less than three months after commencing).15 Large effects (greater than 20 points on a 100-point pain scale) on pain were not observed even at high doses (morphine equivalent dose, 200 mg per day) of an opioid analgesic, challenging the common perception of opioids as powerful analgesics in chronic low back pain.
Although the findings reveal that many people are likely to experience modest pain relief with these medicines, it is important to note these are average effects. Some may experience a larger benefit, while others experience no benefit. The review found that a large proportion of people with chronic low back pain do not respond to opioid analgesics or experience adverse events while taking them, and in half of the studies about 50% of participants dropped out for these two reasons.15 None of the studies evaluated in this systematic review provided data on long-term outcomes.
The risk of adverse events with opioid analgesics is high. Common adverse events include central nervous system adverse events (e.g. headache, somnolence, dizziness), gastrointestinal tract adverse events (e.g. constipation, nausea, vomiting) and autonomic adverse events (e.g. dry mouth).15 However, opioid analgesics are also associated with more serious risks, including dependency, hyperalgesia, tolerance, opioid overdose and death.16-24 There has been a rise in opioid use disorders, diversion of prescription opioids to the illicit market and opioid overdose deaths concomitant with the increase in opioid analgesic prescribing.25-28 About 62 people die each day in the USA from prescription opioid overdoses, with fentanyl misuse cited as a major cause for concern.29 In Australia, there was a 22-fold increase of oxycodone supplied under the PBS between 1997 and 2012, and an increase in oxycodone-related deaths in recent years.30-33 Many oxycodone prescriptions originate from hospital settings for the treatment of acute pain, including acute low back pain.31,34 However, this practice is potentially problematic, and up to 10% of patients prescribed an opioid analgesic in a hospital setting for treatment of acute pain still use an opioid 12 months later.32,35-37 Such trends have prompted major interest in strategies to reduce opioid analgesic prescribing for noncancer pain conditions such as low back pain.
Recommended management of chronic low back pain
In the USA, more than half of people regularly treated with prescription opioid analgesics have chronic low back pain.14 However, an important clinical problem with opioid analgesics is the loss of analgesic efficacy after long-term or repeated dosing. Therefore, an essential approach to managing chronic low back pain is to combine short-term use of opioid analgesics with nonpharmacological interventions aimed at improving function and pain in this condition, such as exercise and physiotherapy.38
Increasingly, evidence around chronic low back pain management supports a patient-centred approach to care within a biopsychosocial framework, as it is unlikely such complex cases can be adequately managed by pharmacological treatments alone, or by a single clinician acting independently.39 The biopsychosocial model of care recognises the complex interplay between psychological, social and biological factors that contribute to illness progression and management decisions.40 With this model, there is the opportunity to address any concerns or incorrect beliefs the individual has about their condition. It is also important to provide patient education. Providing access to pain management resources (e.g. self-help sites) and the accompaniment of written educational material may serve to reinforce verbal advice.41,42
Further to this approach, the use of an opiate risk screening tool is encouraged in the routine management of people with low back pain.43 There should be agreement regarding opioid treatment as part of a multimodal treatment plan, where goals are set based on improved function, there is clear agreement with regard to the provision and dispensation of the opioid (e.g. by one prescriber and one pharmacy, respectively) and there are no replacements for lost repeats and no early repeats. These strategies are in accordance with the Australian and New Zealand College of Anaesthetists Faculty of Pain Medicine opioid treatment plans for chronic noncancer pain and should similarly be adopted for the management of chronic low back pain.43
Unfortunately, it is not always clear what strategies should guide the provision of effective analgesia among individuals who are opioid dependent.16 However, pharmacotherapy with substitution opioids (e.g. methadone liquid or sublingual buprenorphine) is an evidence-based approach that facilitates pharmacological stabilisation of dependence and gives the treating doctor the chance to engage patients in long-term care plans.44
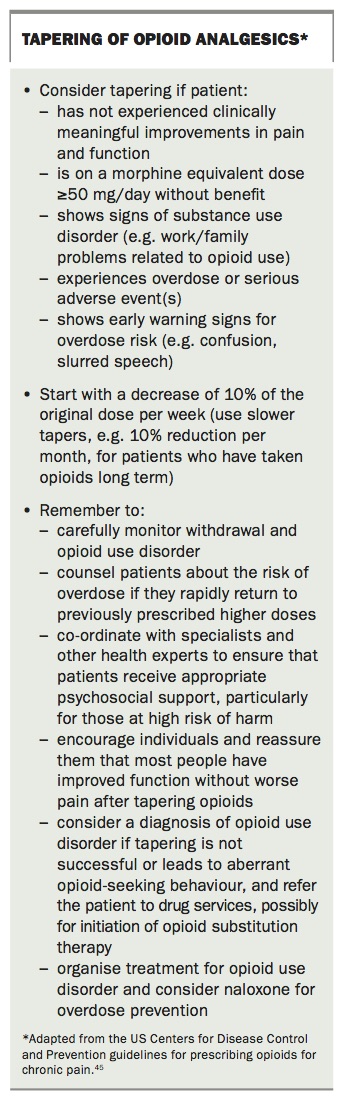
Cessation of opioid analgesics is an expectation during the management of chronic low back pain. The US Centers for Disease Control and Prevention guidelines for prescribing opioids for chronic pain recommend that the opioid analgesic dose should be reduced or tapered down to cessation in certain circumstances, described in the Box.45 Tapering strategies and a summary of the recommended care pathway for patients with chronic low back pain are shown in the Box and the Flowchart.
{kind=link}
Recommended management of acute low back pain
There are several considerations with regard to prescribing opioid analgesics for acute low back pain. First, there is no clinical trial evidence to guide dose or duration of use of these medicines in patients with acute low back pain. Opioid dependency is another concern, particularly among people with a history of abuse, mental health conditions or substance use disorders. Initially, a trial of simple analgesics should be considered, in combination with nonpharmacological strategies that have been shown to reduce pain and facilitate recovery from acute low back pain, such as applying heat packs and engaging in regular activity.9,10 After assessing the patient for red flag conditions (excluding potential serious underlying causes) doctors are encouraged to reassure the patient of the favourable prognosis for acute low back pain.46 Assessing patient motivation and providing assurance of a favourable prognosis where appropriate are integral to the overall management of nonspecific low back pain, particularly as catastrophising and fear-avoidance beliefs among patients with low back pain have been implicated in the transition from acute to chronic pain.47,48 Conversely, well-motivated patients are not likely to experience long-term complications and are more likely to take up the recommended care that has been proven to speed recovery from low back pain compared with other interventions.49
Imaging and bed rest is not recommended for this condition and may delay recovery.9,10 In situations where an individual has not responded adequately to treatment with simple analgesics or has a contraindication to such analgesics, it may be appropriate to consider an opioid analgesic. In such cases, only a short-term course is recommended and the opioid analgesic should be weaned and ceased at the end of the agreed treatment period.50 Further to this, patients should have regular follow-up assessments, be closely monitored for adverse events and set realistic goals for managing their pain and function.51 A summary of the recommended care pathway for patients with acute low back pain is included in the Flowchart.
The need for more evidence
To date there have been no placebo-controlled clinical trials evaluating the efficacy and safety of opioid analgesics in people with acute low back pain. A team of researchers in Australia are currently recruiting participants for the first randomised, placebo controlled trial investigating the use of a short course of opioid analgesia for the management of acute low back and or neck pain (the Opioid Analgesia for Acute Spinal Pain [OPAL] study).52 The trial is investigating use of a time-limited course of an opioid with a clear plan to cease the medicine within six weeks. During the study, the participants are closely monitored by their treating physician and the OPAL research team. General practitioners are able to contribute to new evidence on the efficacy of opioids by being involved in OPAL (sph.opal@sydney.edu.au), and can earn CPD points.
Summary
Although opioid analgesics are commonly prescribed for low back pain, there is limited evidence to support their use. They have shown modest benefits for treating chronic low back pain, yet there is no evidence to guide the use of opioid analgesics for acute low back pain. It is important that if opioid analgesics are prescribed, tolerability and adverse effects are carefully monitored. Long-term use is discouraged and should be accompanied by nonpharmacological therapy, with consideration given to opioid reduction, tapering or cessation. MT
Acknowledgements
Dr Abdel Shaheed received an Early Career Development Fellowship through the University of Sydney School of Public Health. Dr Mathieson receives Fellowship support from an NHMRC Program Grant (ID 1113532). Professor Maher receives an NHMRC Principal Research Fellowship (ID 1103022); NHMRC Program Grant (ID 1113532). Associate Professor Lin receives an NHMRC Career Development Fellowship (ID 1061400).
Professor McLachlan has received grants from National Health and Medical Research Council, Australia for clinical trials on low back pain and sciatica. These trials have also had medicines and placebos supplied by Pfizer Australia and GlaxoSmithKline. Dr Lin has received nonfinancial support (providing the study medication pregabalin and a matching placebo for an investigator-initiated trial that Dr Lin led) from Pfizer.
Dr Maher has received a personal fee from Pfizer for a video seminar on low back pain.