Infiltrating lobular cancer missed on screening mammography

Women's health
A 60-year-old woman has recently undergone mammography screening with normal results; yet, on physical examination, her GP detects a definite lump. Mammography screening for breast cancer is not without pitfalls, so how should women and their GPs approach breast screening?
Case scenario
Marissa, a 60-year-old woman, has had regular two-yearly screening with BreastScreen since the age of 50 years. She has had less regular physical examinations of her breasts. Her last mammography result was normal three months ago, but the GP has noticed a definite lump in her left breast. Investigations show that this is an infiltrating lobular carcinoma.
Commentary
Breast cancer is the most common noncutaneous malignancy in women. In Australia, around 17,000 women are now diagnosed annually.1 After infiltrating ductal carcinoma - not otherwise specified (IDC), infiltrating lobular carcinoma (ILC) is the second most common subtype of breast cancer and comprises 10 to 15% of cases.
There are four main subtypes of ILC:
- classical (by far the most common)
- pleomorphic
- alveolar cell
- solid type.
Sometimes there is a prominent signet cell component. Classical ILC is characterised by its histological appearance of single-file cells percolating through the breast tissue. More commonly than other subtypes of invasive breast cancer, ILC expands by this process rather than forming mass lesions. This is in part because of the lack of the cellular adhesion molecule E-cadherin. A negative result from immunohistochemical staining specific for E-cadherin can be used to support a diagnosis of ILC.
Because of the lack of mass formation some ILC can present with a more global change in the breast, with limited or no typical diagnostic changes detected using mammography or ultrasound. In this situation, there is characteristically an underestimate of the extent of disease by conventional imaging. Hence, when a woman with a symptom presents to the screening program and only undergoes mammography there is a reasonable chance of a false-negative result, especially if she also has dense breast tissue.
Assessment
The situation described here and highlighted by Marissa’s case emphasises the importance of not relying completely on the mammography findings and the importance of triple assessment when there is a breast lump or global change in the shape of the breast. Therefore, the GP correctly sent Marissa for further investigation. Presumably this was initially for an ultrasound and core biopsy of the definite lump. In this type of situation, when there is a proven breast cancer but lack of correlation between clinical and radiological findings, breast MRI can be a useful adjunct to estimate the extent of the breast cancer. Unfortunately, to date, the Medical Services Advisory Committee has not approved diagnostic MRI for funding under the Medicare Benefits Schedule despite several applications, and hence the cost is borne by the patient.
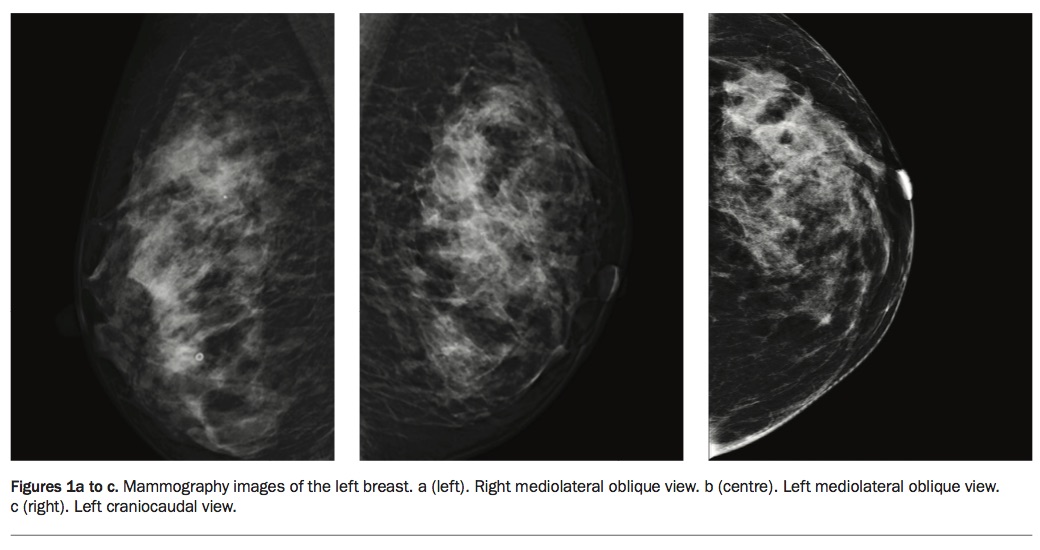
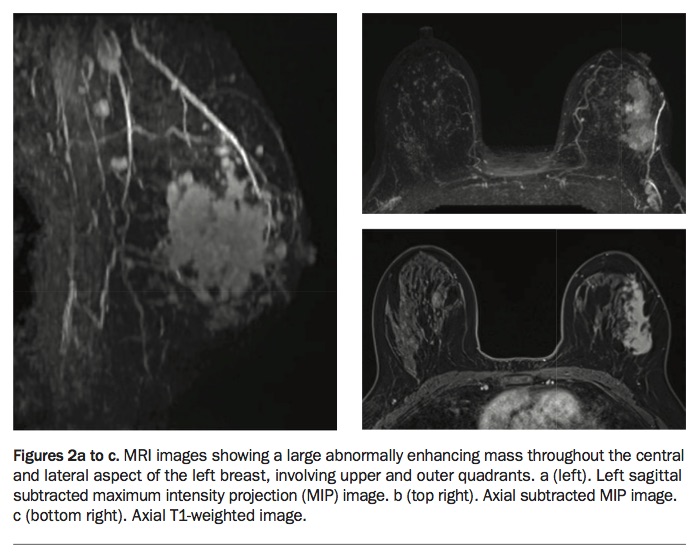
Marissa’s mammography images (Figures 1a to c) are the right and left mediolateral oblique views and the left craniocaudal view, which show no obvious mass or abnormality. The left breast ultrasound (images not included) showed diffusely heterogeneous, dense tissue, but no discrete mass. Her MRI films (Figures 2a to c) show a large abnormally enhancing mass throughout the central and lateral aspect of the left breast, involving upper and outer quadrants, consistent with the whole area being ILC.
{kind=link}
{kind=link}
The role of screening mammography
Screening mammography is by far the best currently available imaging tool for economically viable screening of the whole ‘normal risk’ population of women. BreastScreen Australia actively invites women second yearly from 50 to 74 years of age, but women can attend from 40 years and after the age of 74 years.
The sensitivity for detection of breast cancer by screening mammography is not perfect. The BreastScreen program’s sensitivity for breast cancer detection, using the rate of interval cancers as a reflection of ‘missed’ tumours and measured over 12 months after a normal screening mammogram result, is 87.3% for women who are 50 to 59 years of age. For women aged 60 to 69 years and over 70 years it is 90.8% and 92.4%, respectively. Sensitivity is lower in younger women (40 to 49 years, 79.5%).2
This ‘missed’ cancer rate includes true missed cancers, mammographically occult cancers and cancers that were not present at the time of the screening mammogram but have developed in the interval since (an expected occurrence). Limitations to sensitivity include high breast density (more common in younger women) and distracting lesions such as multiple cysts or fibroadenomas.
As discussed here, certain phenotypes of breast cancer, in particular ILC and noncalcifying ductal carcinoma in situ, are more often mammographically occult.
Recall for assessment is more likely to occur the first time a woman attends for screening mammography because pre-existing lesions are not known about and may need to be confirmed to be benign. Reviewing films from earlier investigations may avoid unnecessary biopsy.
Screening is designed for women who do not have breast symptoms, and it is important that women with a definite symptom such as a new lump or a nipple discharge are not referred to BreastScreen. There may be a delay of up to two weeks between having a screening mammogram and being recalled to an assessment clinic, and women with significant symptoms may experience anxiety because of this delay. Also, a false-negative screening mammography result in a woman who has breast cancer symptoms may lead to false reassurance and further delay to diagnosis.
ILC is often diagnosed using standard mammography, appearing as a focal change or pattern distortion, and often there is correspondence between the imaging findings and the final histological parameters. However, as in Marissa’s case, normal mammography findings despite the presence of cancer are more common with ILC than IDC. Ultrasound and MRI can also underestimate the extent of an ILC or, sometimes, other subtypes of breast cancer.
Conclusion
Assessment of the extent of a breast cancer clinically and radiologically is best done in the context of an experienced multidisciplinary team including specialised breast imaging radiologists and an expert surgeon or breast physician for clinical assessment and integration of the information. It is important to have access to contemporary imaging technologies such as mammographic tomosynthesis and breast MRI.
Breast self-examination is not an effective screening tool.3 Despite this, all women should be familiar with their breasts and report any new symptoms to their GP. If a patient has breast symptoms it would be good practice for their GP to examine the breasts and not just send the patient for imaging. Women should have regular screening with mammography from 50 years of age via BreastScreen. If they are at higher risk of developing breast cancer or if they have very dense breast tissue they should consider annual mammographic (preferably 3D tomographic, if available) and ultrasound imaging, perhaps from 40 years of age depending on their specific circumstances. MT