Pain in advanced cancer. Next steps in successful pain management

Dr Ramachenderan is a Palliative Care Senior Medical Officer and GP Anaesthetist at Albany Health Campus, Albany. Associate Professor Auret is a Palliative Care Physician and Academic at The Rural Clinical School of Western Australia, Albany, WA.
Cancer pain
Pain
Pain in advanced disease is a multidimensional experience that can significantly impact on quality of life. Although pharmacotherapies are the cornerstone of managing pain in advanced cancer, other biological and nonpharmacological therapies can be used in conjunction to further relieve pain. A multidisciplinary and holistic approach that encompasses nonpharmacological and pharmacological therapies can enhance pain relief in patients with advanced cancer.
- Pain is a dynamic and multidimensional experience that is best treated using social-psychological-spiritual-biological management strategies.
- Psychosocial and spiritual distress can worsen a patient’s experience of pain, and addressing these are key factors in successful pain management.
- Multimodal therapy is the mainstay of pharmacological pain management in advanced cancer.
- Pre-existing organ dysfunction, medication side-effect profile and patient social and psychological factors must be considered when selecting pharmacological therapies.
In advanced disease, a multidisciplinary team is best placed to provide social, psychological, spiritual and biological management of total cancer pain for patients and their families, and early referral to a specialist palliative care team is recommended.1-5 In the first article of this series, we explored holistic assessment as the first step in successful management of pain in advanced cancer. We described how pain is a multidimensional experience and discussed the dynamic relationship between social, psychological, spiritual and biological factors that result in total pain.6 In this paper we use the same framework to discuss specific interventions for managing pain in advanced cancer, allowing for the individuality of each patient’s experience to be recognised and responded to.
Social and psychological interventions that assist cancer pain management
There are four key psychosocial strategies that are useful in managing pain in patients with cancer:1-4,7
- identify and treat psychological distress
- improve a patient’s ability to cope with pain
- improve self-efficacy to manage pain
- strengthen social supports.
Identify and treat psychological distress
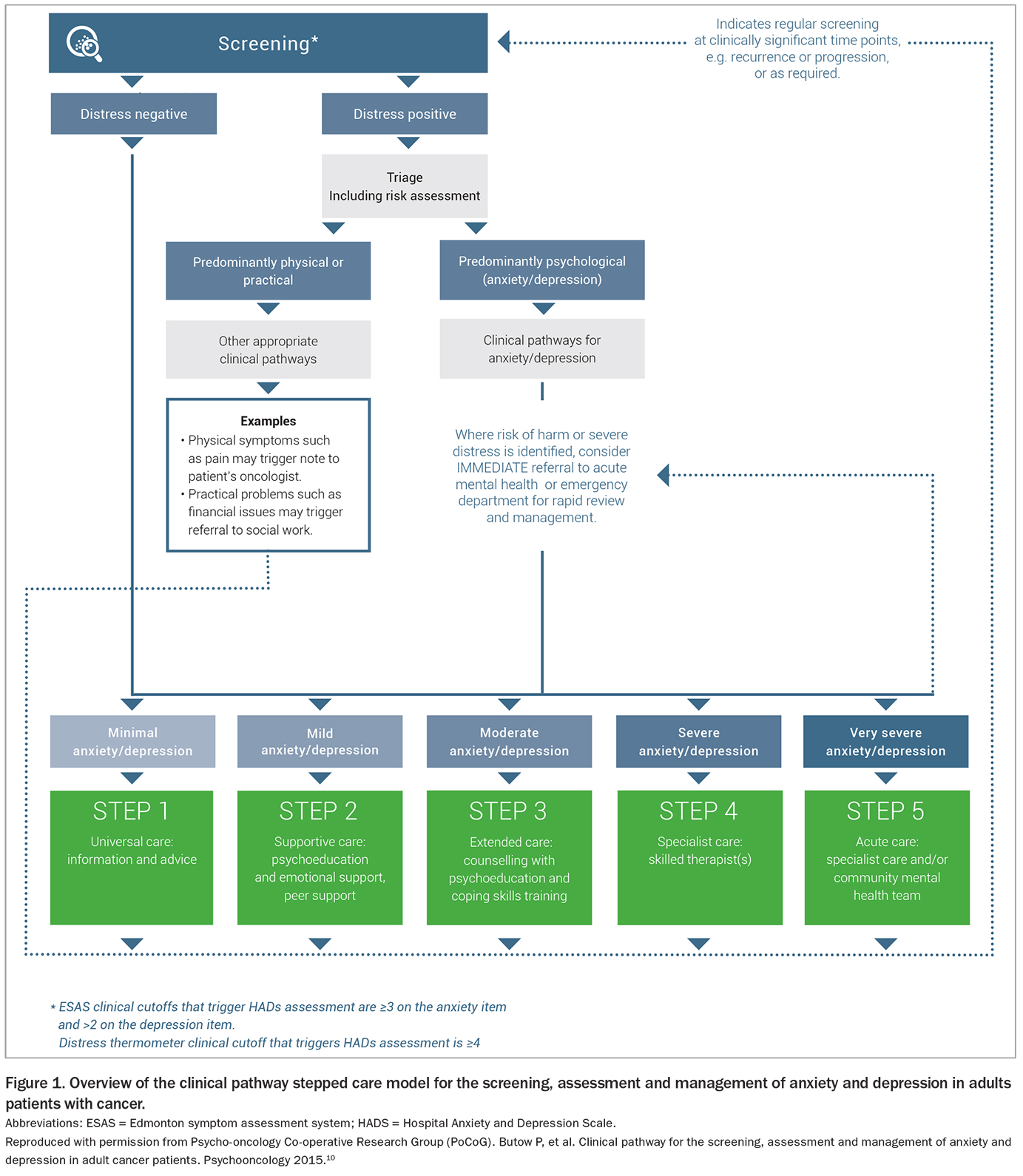
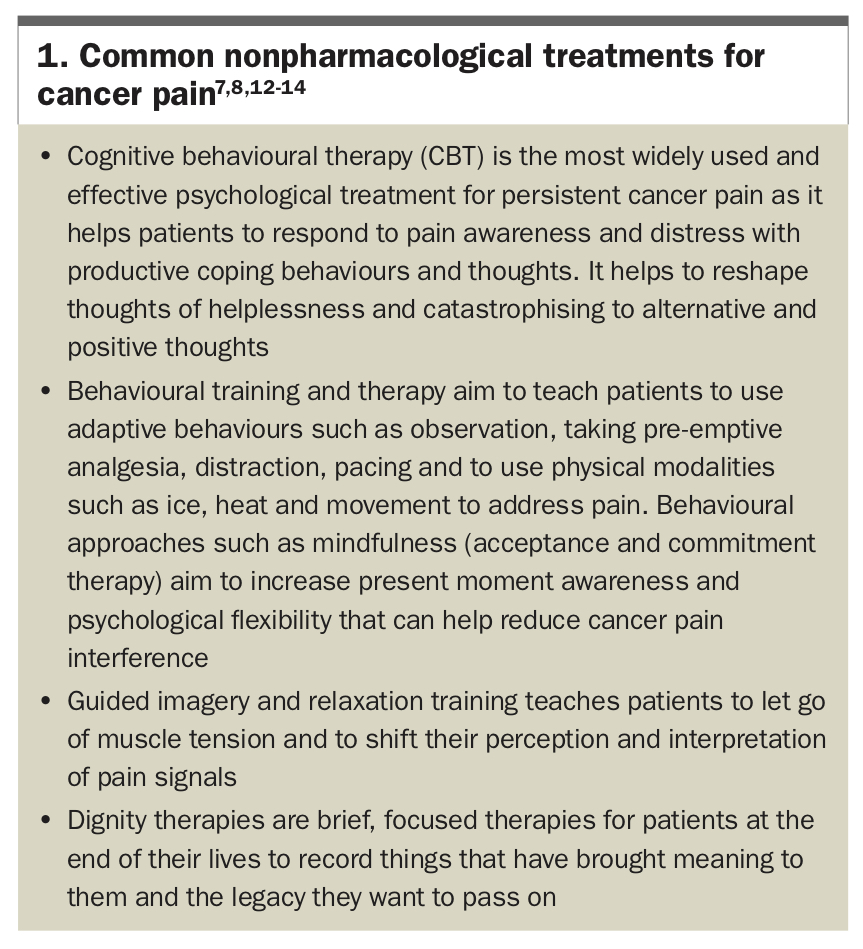
Identification and treatment of premorbid and illness-related low mood, anxiety and depression can have a very significant effect in optimising analgesic therapy in patients with advanced cancer pain.7 The ‘distress thermometer’ has shown promise as a screening tool with the more detailed Hospital Anxiety and Depression Scale (HADS) used if concerns are identified (www.nccn.org/docs/default-source/patient-resources/nccn_distress_thermometer.pdf?sfvrsn= ef1df1a2_4).8,9 A stepped-care approach should be applied with the least intensive treatment being recommended first (Figure 1).9,10 Cognitive behavioural therapies (CBT) have a comparable effect size to some analgesics and should always be considered in psychological cancer pain management (Box 1).7,8,11-14 At all times suicidality should be considered and acted upon appropriately.
{kind=link}
{kind=link}
Patients with mild to moderate depression can benefit from online or face-to-face CBT and peer support groups. Individual psychotherapy also may be useful for those with significant emotional distress. Pharmacological management may be required for those who do not respond to the stepped approach, with selective serotonin reuptake inhibitors (SSRIs) or serotonin noradrenaline reuptake inhibitors (SNRIs) the preferred therapies over tricyclic antidepressants due to their favourable side-effect profile. Mirtazapine is often prescribed for patients in palliative care due to its effectiveness in improving sleep quality and weight gain.15 Consideration must be given for medication side-effect profiles, potential drug interactions and patients’ pre-existing comorbidities.8,9 Other important psycho- oncology resources include booklets on emotions and cancer by the Cancer Council (https://www.cancer.org.au/assets/pdf/emotions-and-cancer-booklet) and Beyond Blue (https://www.beyondblue.org.au).
Psychological distress in cancer pain also encompasses emotional distress, fear and worry, which are amenable to cognitive and behavioural approaches and relaxation and guided therapies (Box 1).2, 7,14
Improve coping ability
Pain catastrophising is ‘the tendency to focus on and exaggerate the threat value of painful stimuli and devalue one’s ability to deal with pain’.3,7 In patients who have this tendency, CBT can help reduce this response by reframing catastrophic thinking and promoting adaptive behaviours and self-efficacy.
Attention-diversion is another method of enhancing coping skills. High quality evidence shows that relaxation training and guided imagery, together with pain self-management education, can be effective in reducing pain when used with a pharmacological regimen.7 Behavioural approaches such as mindfulness meditation, diaphragmatic breathing and engaging in meaningful and stimulating activities with friends and family have also been shown to be effective tools.1
Improve self-efficacy to manage pain
Patients who report and demonstrate a high level of self-efficacy to manage their pain, report lower levels of pain.4 Therefore, improving a patient’s confidence through pain and medication education and identifying barriers to pain control can help reduce their pain.7,11
Complimentary to education are practical enablement strategies, such as medication prompt lists, pain scales and diaries, pain management and function goals, cue cards, provision of weekly pill-boxes, phone support, video or MP3 cognitive and relaxation exercises and a personalised pain management plan.11
Strengthen social supports
Social interventions for patients with cancer pain must focus on supporting and enhancing the closeness of the carer-patient relationship. This can be achieved through improving carer understanding of the disease process and pain education, providing respite and support services for carers and consistently affirming the carer role.4 There is also evidence to show that a strong partner or marriage relationship can improve a patient’s cancer pain as well as their and their partner’s quality of life.16
One key measure that can help patients better manage their pain is referral to a social worker who can help identify any social, cultural, financial or spiritual barriers. Social workers assist pain management by facilitating communication between treating health practitioners and patients; assessing family resources (financial, social, relational); highlighting strengths and limitations to being able to provide care; providing psychological support; and using a problem solving-approach that incorporates a patient’s environmental resources.17
Additionally, community public health support programs such as Compassionate Communities allow health professionals to work in partnership with civic and personal patient networks to support patient and carers at home, especially with end-of-life care.18 Engaging communities can help carers by decreasing fatigue, helping with practical aspects of care, improving learning and carer personal growth and increasing social care networks and, thus, social capacity.19
Spirituality and cancer pain
Spirituality is how people find meaning, purpose and hope in their lives. It can be seen as the bedrock in which a person’s physical, psychological and social world are imbedded.20 The expression of spirituality is broad and encompasses various formal and informal practices that allow people to connect to themselves, to the sacred and to the significant.20-23
Spirituality practised in the face of advanced disease and cancer can provide patients with higher levels of function and self-esteem, strength to cope with their illness and peace and meaning during their cancer treatment.21,22,24-26 Spiritual practices can improve the tolerance of pain, but conversely spiritual suffering can influence how a person experiences and expresses pain. Untreated spiritual suffering may worsen the pain experience and can cause greater concern than physical symptoms.21,23,24
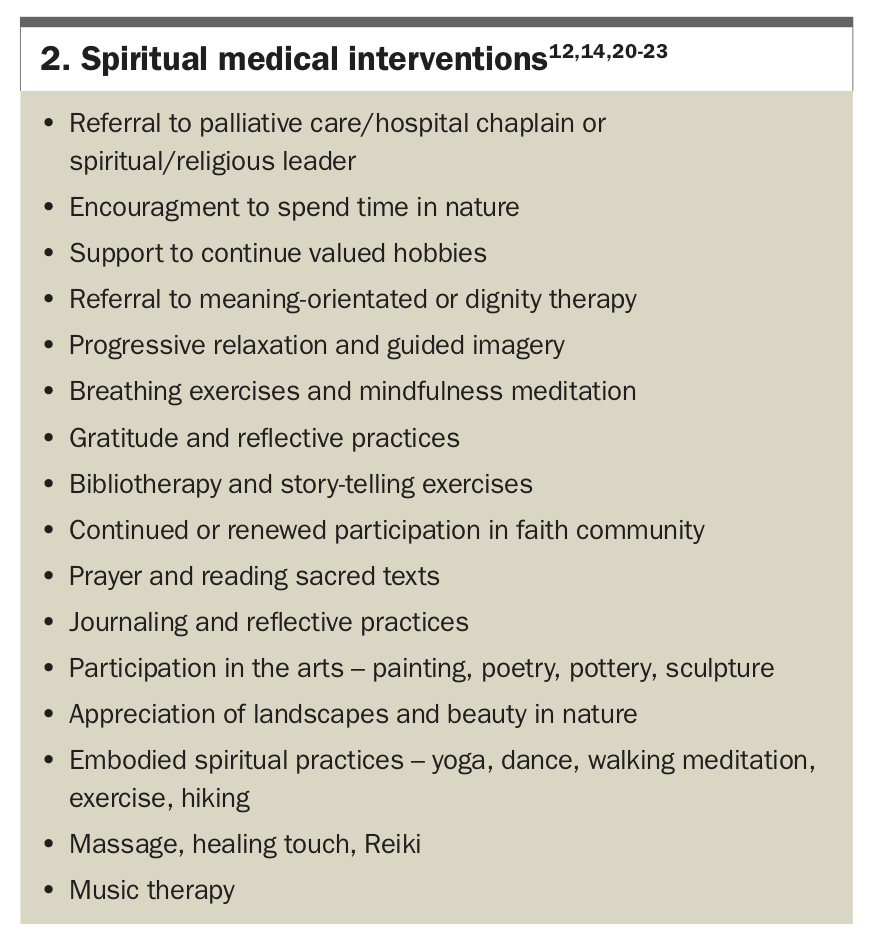
Enquiry is the central aspect for applying spiritual interventions to cancer pain management. Patients’ trust in their doctors increases when their spirituality is addressed, and many patients report that they want spirituality integrated into their treatment.27 The FICA tool and Fitchett and Risk questions can be used to identify a patient’s spiritual needs.28,29 From here, both formal and informal spiritual interventions can be recommended (Box 2).12,14,20-23
{kind=link}
Biological management of cancer pain
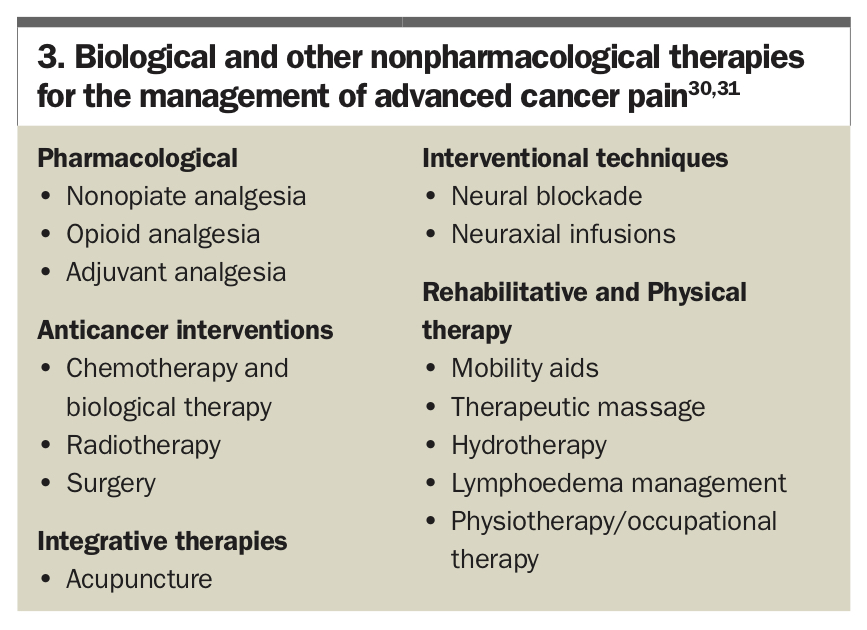
There are numerous effective pharmacological and nonpharmacological biological modalities for managing pain in advanced cancer (Box 3);30,31 however, this review focuses on the pharmacological aspects. Although multimodal pharmacological management is the mainstay of cancer pain, treatment, anticancer treatments such as chemotherapy, radiotherapy (e.g. for painful bony metastases) and surgery (e.g. fixation for pathological fractures) can help reduce pain in advanced cancer.1,30,32
{kind=link}
Pharmacological management of advanced cancer pain
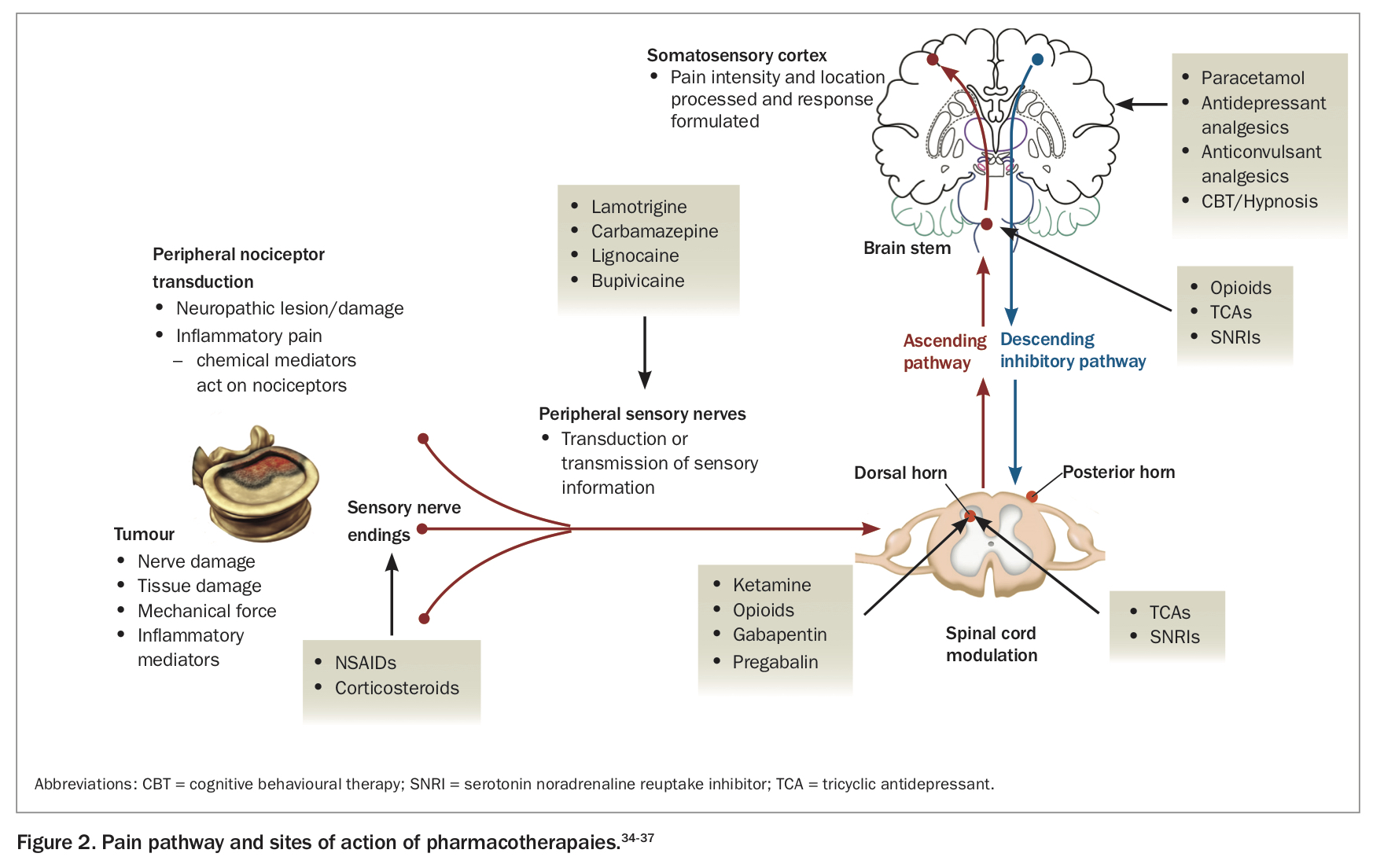
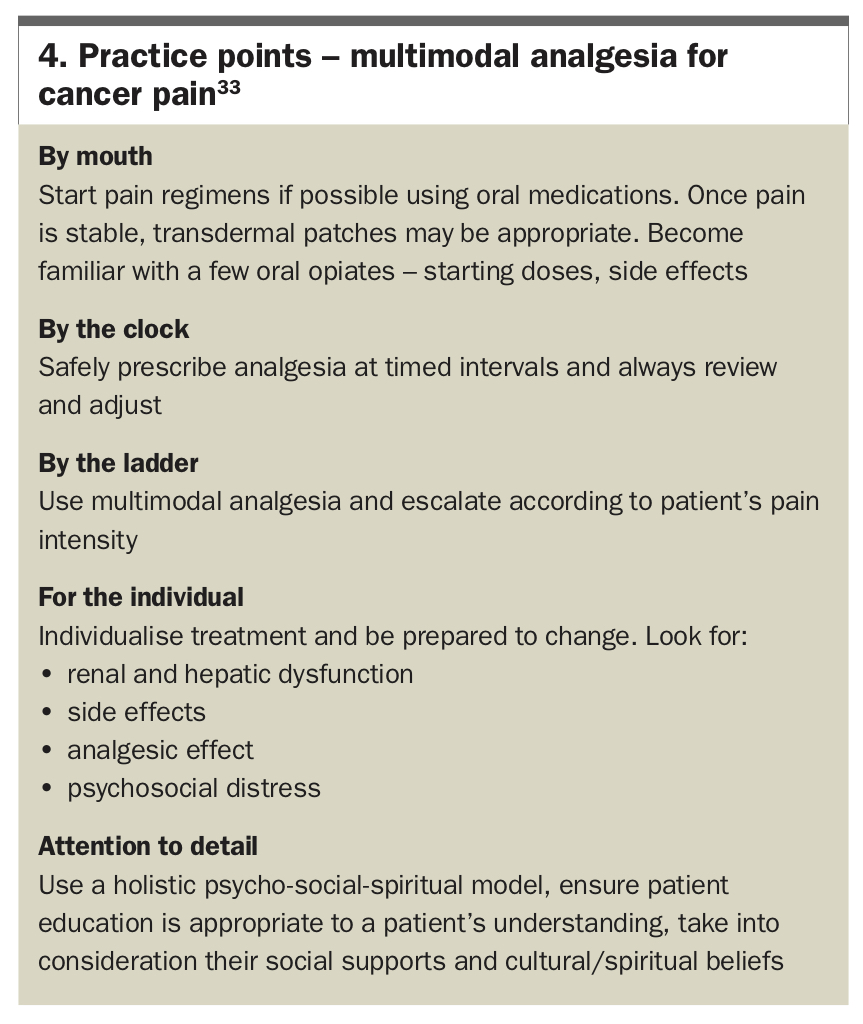
Most cancer guidelines reference the World Health Organization cancer pain ladder33 and promote a stepwise escalation of therapy and a multimodal approach, safely combining medications to target receptors involved in pain transmission (Figure 234-37).38,39 The WHO’s five foundations for the correct use of analgesics to maximise effectiveness are especially relevant and are summarised in Box 4.40 Cancer pain is often a heterogenous mix of nociceptive and neuropathic mechanisms and deciding on the predominant pain type can guide multimodal treatment.41
{kind=link}
{kind=link}
Initiation of multimodal analgesia consists of starting with regular paracetamol and an NSAID when clinically appropriate.42,43 As pain escalates, an immediate-release (IR) strong oral opiate can be used four-hourly and titrated according to a patient’s pain. Additionally, a low-dose, slow-release (SR) opiate can be started if a patient’s pain is frequent and constant. Oral morphine, oxycodone or hydromorphone can be used, depending on the doctor’s experience and familiarity with these medications.44,45 If pain control is inadequate, the four hourly dose can be increased by 30 to 50%, with a double dose at bedtime for more restful sleep.31,32 As the total daily dose of strong opiate use is titrated, it can be converted into a more stable regimen of a daily or twice daily SR opiate or to an opioid transdermal patch.
The combination of a regular SR opiate with an IR as-needed oral opiate for breakthrough pain on a background of regular paracetamol and an NSAID where appropriate and where no contraindications, forms an effective base for advanced cancer pain treatment.32,42,45 If neuropathic pain is suspected as an accompanying factor, adjuvant analgesia with medications such as tricyclic antidepressants or anticonvulsants can be added to enhance the effects of the primary analgesics and reduce the need for high opioid doses.46,47
The nuances of treatment can be finessed with time through regular review and adjustment of the regimen to manage neuropathic pain, opioid-related side effects, symptoms of progressive disease, refractory pain and pronounced patient and carer suffering and distress.46
Paracetamol and NSAIDs
Both paracetamol and NSAIDs inhibit prostaglandin formation and can be useful in somatic pain and for opioid-sparing effects.38,39,42-44,48 Paracetamol may be less beneficial for patients receiving regular opioids and may be ceased if there is a high pill burden.49 The overall daily dose is reduced from 4 g/day to either 2 g/day, or omitted entirely in patients who have renal or liver dysfunction or low body weight/cachexia.42
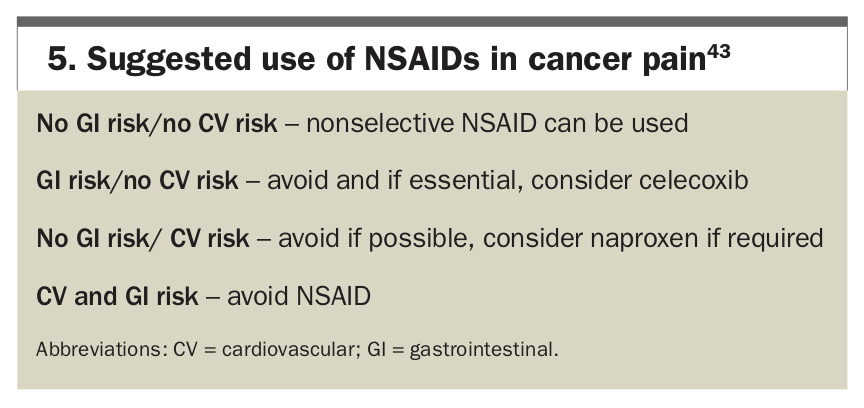
The lowest effective dose of NSAID should be used for the shortest duration and side effects reviewed regularly. It must be used with caution in high-risk elderly patients, those already on corticosteroids or those with renal and gastrointestinal disease.43,45 Care must be taken with respect to the renal, cardiovascular, gastrointestinal and haematological side effects of NSAIDS.30,43 Practice points for the use of NSAIDs for cancer pain are summarised in Box 5.
{kind=link}
Opioids
Opioids are the cornerstone of pharmacological management of advanced cancer pain. The European Association of Palliative Care guidelines recommend that oral hydromorphone, oxycodone or morphine be used as first-line opioids for cancer pain.44 Care must be taken in patients with renal impairment as opioid metabolites are renally excreted and can accumulate and exert continued action, potentially leading to clinically significant neurotoxic side effects such as myoclonus, seizures, oversedation and respiratory depression.50,51
Although morphine has been considered as the standard first choice of opioid for advanced cancer pain, there is no evidence of superior efficacy or safety compared with other opioids such as oxycodone or hydromorphone.31 Therefore, the best opioid is what is tolerated, effective and appropriate to an individual’s circumstances. All other opiates are measured against and draw equivalency to morphine, with its assigned clinical potency of 1.50 It has the advantage of being widely available in a variety of formulations. It is metabolised in the liver into morphine-6-glucuronide, which exerts its analgesic action, and morphine-3-glucuronide, which is responsible for many of its known side effects.
Oxycodone is a synthetic opiate, available in oral and liquid formulations with immediate and long-acting options. It is highly bioavailable with onset of action in 15 minutes.52 Its side-effect profile is similar to morphine with some reports of less nausea and hallucinations.42,43 Oxycodone has also been combined with naloxone to help reduce opioid-related constipation. Liver impairment can impede the first pass metabolism of naloxone thus reducing the central analgesic action of oxycodone.53
Hydromorphone is a preferred first choice of oral strong opioid in patients with advanced cancer and kidney disease.31,54 It is five times more potent than morphine and is used frequently for subcutaneous pain relief in the terminal phase if large amounts of oral morphine equivalents are required.42,50
Fentanyl is a highly potent and lipophilic opiate that can be used via parenteral, transdermal, neuraxial and transmucosal routes.31,39,50 Transdermal fentanyl is considered for patients with chronic stable cancer pain who have a high pill burden or prominent gastrointestinal symptoms. It offers a reliable 72 hours of analgesia.31 Because it can take 12 to 24 hours to reach steady state, it is not appropriate for patients with unstable pain.43 Care must be taken with opioid-naive patients as the lowest dose patch delivers 12 mcg/h, equivalent to about 40 mg oral morphine per day.
Transmucosal fentanyl via the sublingual route is approved for use in cancer pain. It is particularly useful for incident pain induced by bone metastases and troublesome breakthrough pain due to rapid mucosal absorption.44,55 Its use should be guided by specialist providers to ensure safe titration.
Buprenorphine is available in transdermal and sublingual preparations and is used in the treatment of opioid addiction at high dosages and in chronic noncancer pain.31 Via the transdermal route it takes 12 to 24 hours to produce analgesia, with steady state reached in one to three days.43 It is used in opioid-naive patients with cancer pain and has the advantage of less constipation and a ceiling effect on respiratory depression.50
Tapentadol is novel agent that may be effective for both nociceptive and neuropathic cancer pain.43 It acts both as a mu opioid receptor agonist and a noradrenaline reuptake inhibitor. A Cochrane Review found that tapentadol was no more or less effective or tolerated in the treatment of cancer pain compared with morphine and oxycodone.56 It offers a better side-effect profile, with fewer gastrointestinal effects (nausea, vomiting, constipation) compared with pure mu agonists. One limitation to tapentadol’s role in advanced cancer pain may be the limit of dose escalation in patients with progressive disease, with few studies published with doses exceeding 500 mg/day.57
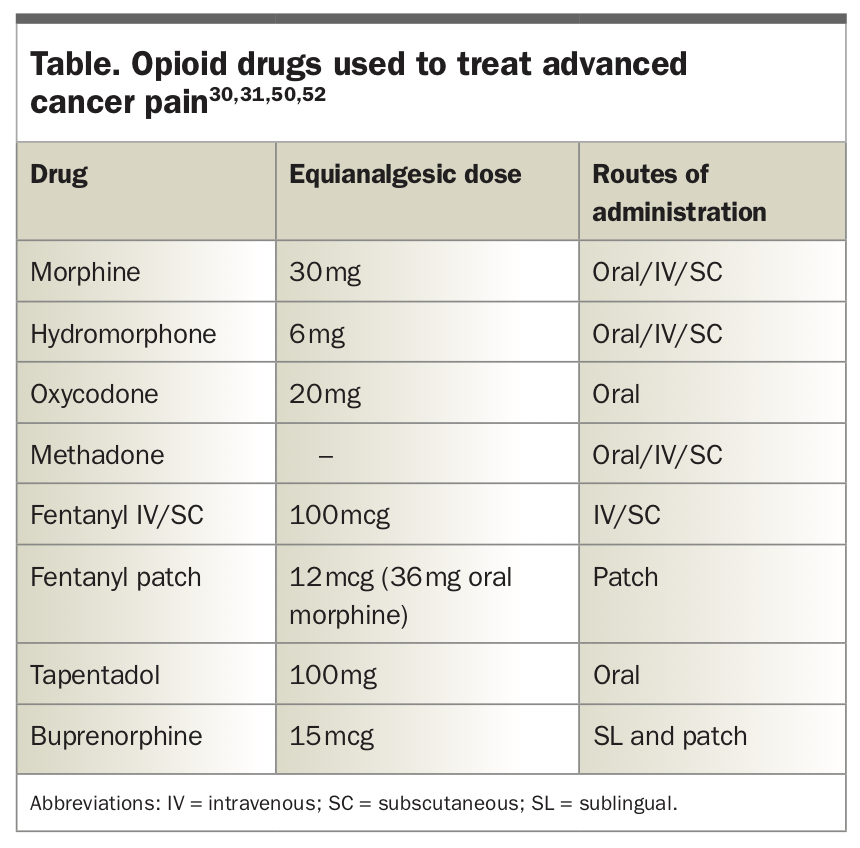
Methadone is a unique and potent opioid that is usually reserved for patients with difficult to control neuropathic and nociceptive cancer pain.39,42,58 Its pharmacokinetics are highly variable and, therefore, in switching from another opioid, its use should be guided by specialist providers.31,49,58 As it does not have any active metabolites, it can be used in patients with kidney disease; however, it can prolong the QT interval and lead to significant sedation.54,59 It also known to interact with common medications including omeprazole and selective serotonin inhibitors (Table).30,32,42
{kind=link}
Breakthrough pain
For patients experiencing breakthrough pain (pain with no trigger), an appropriate ‘as needed’ dose of opioid can be calculated as one sixth of the total daily oral morphine equivalent dose.60
Example: Mrs CM is taking oxycodone SR 30 mg twice daily (total oral morphine equivalent of 90 mg). Her breakthrough dose of oral IR oxycodone is 10 mg every three to four hours.
For patients using transdermal fentanyl or buprenorphine who have breakthrough pain, oral IR oxycodone, morphine or hydromorphone can be used in proportion to the patient’s total opioid dose.43
Example: Mr JR is on a fentanyl patch 25 mcg/h (total oral morphine equivalent of 75 mg). His breakthrough dose of opiate could be either oral IR morphine 12 mg, IR oxycodone 8 mg or hydromorphone 2 mg.
Opioid side effects
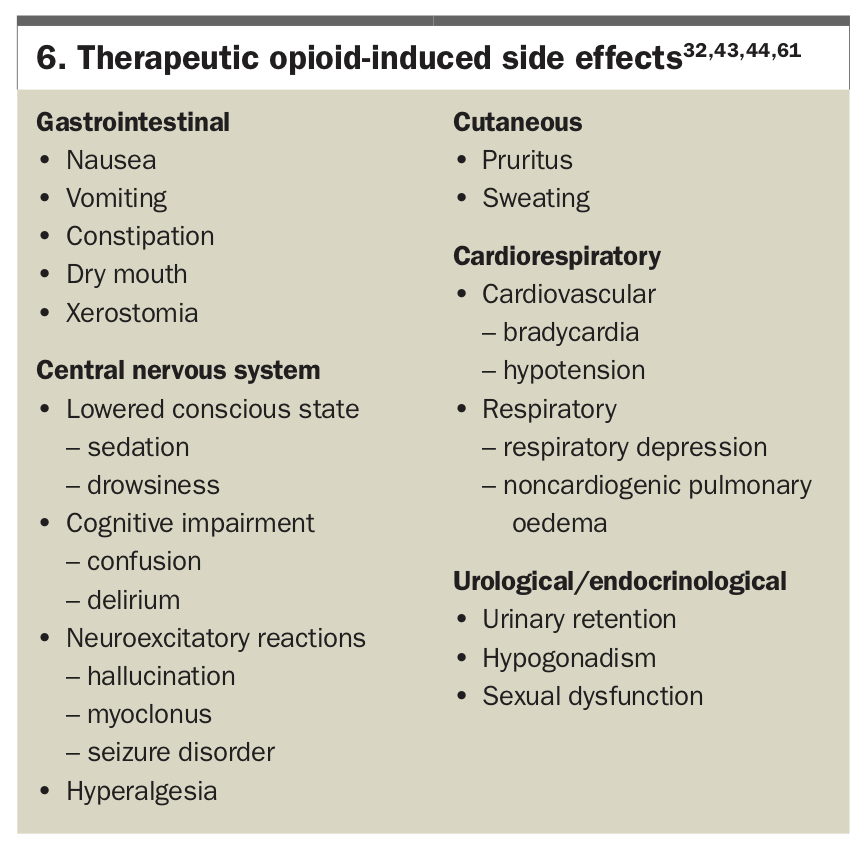
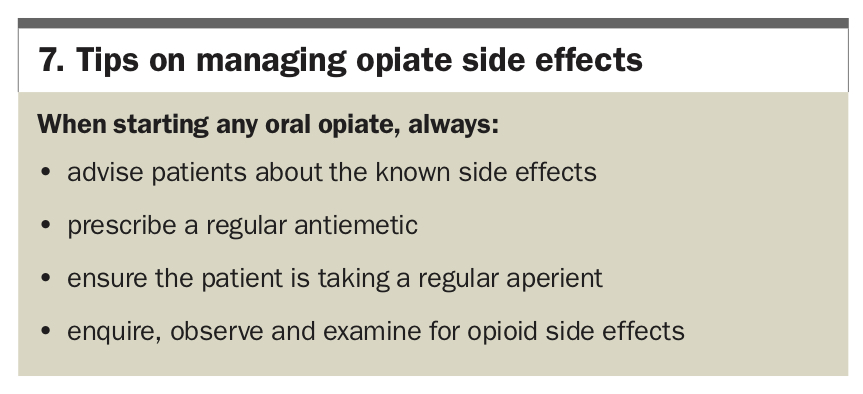
Clinicians must routinely ask about opioid-related side effects, especially constipation, drowsiness, nausea and vomiting, and treat these effectively to improve adherence to an analgesic plan.30-32,42 Common therapeutic opioid-induced side effects are listed in Box 6.32,43,44,61
{kind=link}
Opioid-related constipation is common and worsened by immobility, older age and low oral intake.30 All patients require a regular prophylactic stool softener and stimulant laxative, such as docusate and senna.42,55 Bulking agents, such as fibre supplements, are not effective and can cause bloating and lower abdominal pain. Methylnaltrexone, a subcutaneous peripheral opioid antagonist, can help as rescue therapy when regular aperients have proven to be ineffective but prevention is the preferred path.30,42,44
Nausea and vomiting are experienced by up to 40 to 60% of patients starting opioid therapy.32,44 Use regular antiemetics (e.g. metoclopramide or haloperidol) for a few days until tolerance develops. Other options for ongoing nausea are using an alternative opioid, reducing the dose or changing the route of administration.42,44
Drowsiness is very common at therapy initiation or dose increase, but usually resolves in a few days. If drowsiness is persistent and starts to affect normal activities, an opioid rotation or lowered doses can be considered.30,32,42
Opioid-related neurotoxicity (myoclonus, confusion, delirium, hyperalgesia and/or seizures62) must be recognised early so management can occur correctly. The management of neurological side effects usually involves four key measures: reducing the overall opioid dose by 25 to 50%, considering an opioid rotation, ensuring proper hydration to promote excretion of metabolites and using adjuvant medications to reduce opioid consumption while providing comfort.43,63
Opioid-induced hyperalgesia (OIH) is a paradoxical phenomenon where patients experience an increase in diffuse pain and show a heightened responsiveness to painful stimuli that does not improve with increasing opioid doses.30,43,61 OIH may occur when patients have had a rapid increase in opioid dose and/or have been using high doses of opioids for a long duration. Chronic opioid use typically induces tolerance (increased dose for same response) but in OIH, an increased dose results in worse pain. Mechanistically, this is thought to involve a combination of microglial cell activation, N-methyl-D-aspartate receptor activation, glutaminergic activation and alteration in intracellular opioid signalling.64 Managing OIH involves education, ensuring proper hydration, considering an opioid dose reduction by 25 to 50%, considering an opioid rotation and optimising the use of adjuvant medications (Box 7).
{kind=link}
Neuropathic pain agents
For patients with cancer-related neuropathic pain or mixed neuropathic pain, opioids alone are unlikely to provide effective pain relief. This is likely to be associated with significant side effects due to the high doses required. Adjuvant medication for neuropathic pain can provide more effective pain relief.43,45,56,65 There are multiple adjuvant medications available including amitriptyline, nortriptyline, gabapentin, pregabalin and duloxetine.32,42-45,66-68 If the first treatment choice is ineffective or side effects are unacceptable, second-line treatment should come from one of the remaining first-line medications.65 Nortriptyline may be a better option for some patients as it has a better side-effect profile.
The choice of agent is guided by availability, ease of dosing, pre-existing organ dysfunction (using pregabalin with caution in patients with renal failure), side-effect profile (nortriptyline and amitriptyline may help with insomnia) and aetiology of neuropathic pain (duloxetine is indicated for chemotherapy-induced peripheral neuropathy).43,67,69
Adjuvant medications are commenced at low doses with gradual up-titration according to pain response and side effects. It can take several days for pain to improve therefore judicious titration is indicated.66,67
Lignocaine patches can be used topically to relieve focal and persistent neuropathic pain and allodynia.38,70 A patch can be placed over the painful area for 12 hours and removed for 12 hours. With 3% of the patch being systemically absorbed, it is useful for older patients and high-risk groups; however, the significant cost currently may be prohibitive to some patients.71
Other agents
Corticosteroids
Corticosteroids can be helpful in several cancer pain syndromes, acting to reduce inflammation by inhibiting prostaglandin synthesis and reduce oedema that is associated with tumour growth.72 They are especially useful for pain caused by visceral distention (e.g. liver capsular stretch), emergency management of metastatic spinal cord compression, reducing intracranial pressure and acting to relieve discomfort in malignant bowel obstruction.32,38,48 They can also play a role in cancer bone pain and neuropathic pain.72 Dosing ranges from 4 to 16 mg dexamethasone daily in the morning, depending on the indication, with 8 mg of oral dexamethasone equivalent to 50 mg of oral prednisolone.73 Tapering is recommended if use extends beyond three weeks, with effectiveness being evaluated on the balance of quality of life improvements and side effects with longer-term use.72 Where possible, always aim to use the lowest dose for the shortest time.
Cannabinoids
Medicinal cannabinoids tetrahydrocannabinol (THC) and cannabidiol (CBD) have gained popularity in the past number of years since becoming available in Australia under a special access scheme. Cannabinoid receptors CB1 and CB2 have been linked to the inhibition of pain and THC and CBD interact with other analgesic receptor systems.38,65 However, despite the theoretical promise, the evidence for medicinal cannabinoids in cancer pain is weak and unclear and is, therefore, not endorsed as an effective analgesic on its own but rather as an adjunctive measure.38,65,74,75
Lignocaine and ketamine
There is a growing body of evidence that supports the efficacy of lignocaine infusions for the treatment of refractory cancer pain.76,77 Administered intravenously or subcutaneously using a weight-based dose, lignocaine is infused over a few hours or days in a specialist palliative care inpatient setting for the treatment of OIH and refractory cancer pain.
Ketamine has been used as adjunctive agent alongside opioids in difficult to control pain especially patients with central sensitisation (allodynia and hyperalgesia), refractory neuropathic pain and increasing opioid tolerance.38,45,47,78,79 In the cancer setting, it is most commonly used as a sublingual lozenge or parenterally over a period of hours or days, with doses ranging from 1 mg/kg/h to 600 mg/day.79 However, two Cochrane Reviews have found insufficient evidence of efficacy and a randomised controlled trial of subcutaneous ketamine for refractory cancer pain found increased adverse events but no impact on pain compared with placebo.80,81
Denosumab and bisphosphonates
Cancer bone pain is the most common and troublesome tumour-related pain in advanced cancer, experienced as background, incident (movement-related) and breakthrough pain, reflecting a complex overlap of inflammatory nociceptive and neuropathic stimuli.37,56 Along with opioids and short course external beam radiotherapy for painful localised metastatic bone lesions, bone strengthening agents such as denosumab and bisphosphonates are useful to decrease pain, pathological fracture, need for surgery and spinal cord compression.45,48,82,83
Refractory cancer pain
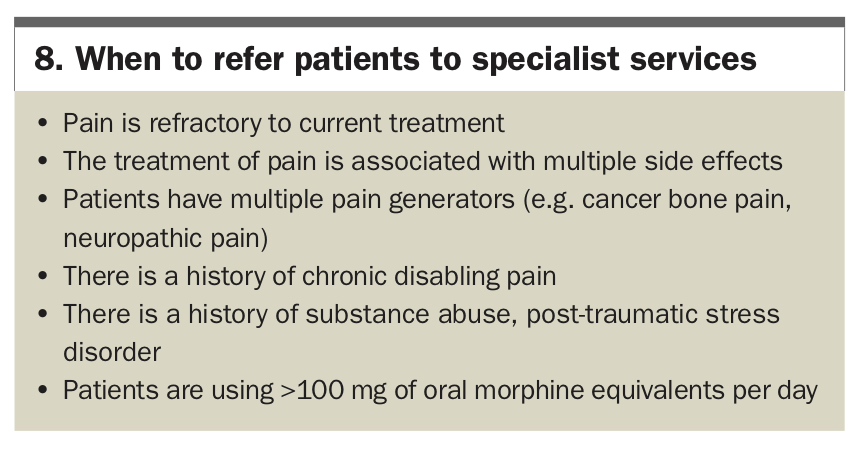
Although most patients with cancer pain achieve reasonable control, between 10 and 20% of patients may not respond to standard therapies.38,45 Risk factors for refractory pain include younger age, history of prior substance or opioid abuse, significant neuropathic pain and psychosocial distress.38 These patients require early referral to specialist pain and palliative care services to enlist a socio-psycho-biological approach to their pain (Box 8).
{kind=link}
For patients with refractory cancer pain, the approach required is a broad review of their analgesic regimen, answering six important questions.38,39,45,47
- Is multimodal analgesia being used? If so, can it be optimised?
- Is neuropathic pain present? If so, how will it be treated?
- Does the patient need an opioid rotation? Are there signs of neurotoxicity?
- Would this patient benefit from adjuvant analgesia?
- Are there any psychosocial issues that have not been addressed?
- Would this patient benefit from an interventional technique such as a nerve block or spinal infusion?
Conclusion
The suffering from pain in advanced cancer can be pronounced and have a lasting impact on a person’s experience and their family’s memories. Providing holistic assessment and personalised management involves the use of the socio-psycho-spiritual-biological model of care. Psychological, social and spiritual interventions can have a profoundly positive impact and work synergistically with a clear and mindful biological treatment plan. A regularly assessed multimodal medication regimen with appropriate adjuvants helps to ensure comfort and allow patients valued time and space with their loved ones. PMT
COMPETING INTERESTS: None.