A young woman with cheek pain after a work injury

Facial injuries and disorders
Pain
A pain specialist discusses the assessment and management of a 28-year-old woman who has shooting pains into her right cheek after a splash injury to her right eye when preparing podiatry instruments for sterilisation. She has several stressors – study, work and planning her wedding – and psychosocial aspects may be more significant in this case than biomedical aspects.
- Assessment and management of patients with persistent pain requires consideration of biomedical and psychosocial factors.
- Once serious and/or easily treatable pathologies have been excluded, the role of nervous system sensitisation in persistent pain should be addressed.
- Return to work is an important treatment goal for people with persistent pain, providing a positive identity, independence, social contact, satisfaction and structure.
- Successfully addressing psycho social factors at a relatively young age can help build the insight and skills needed for lifelong wellbeing.
- GPs have a key role in coordinating care, ensuring appropriate medical and allied health input and encouraging a return to normal function.
Picture credit: © Studiomoment/iStockphoto.com Model used for illustrative purposes only.
Case scenario
Ms AD, aged 28 years, is studying psychology part time at university and until recently was working as a receptionist at a local podiatrist. One of her duties at work was to clean the instrumentation ready for sterilisation. When she was doing this a few weeks ago, some of the debris splashed into her right eye. She promptly rinsed her eye with water and sought review at a nearby optometrist, who reported ‘all clear’.
This incident resulted in continuing discomfort, both physical and psychological, for Ms AD. Convinced that there was something ‘nasty going on’ in her eye she sought further reassurance from her GP, who referred her to an ophthalmologist. Once again she was reassured that there was no likelihood of contamination.
Even though the incident and subsequent follow up was well handled by her employer, who paid for all the reviews, Ms AD resigned from the job fearing another episode. Moreover, since the incident she has had recurrent painful aphthous ulcers in the mouth and a recurrence of cold sores affecting the left upper lip.
Ms AD is now complaining of occasional shooting pains once or twice a day into her right cheek. These only started after the work incident and do not appear to have a trigger. However, as the pain emanates from her right tragus, investigations will need to rule out temporomandibular joint dysfunction.
In the meantime she has agreed to trial an over-the-counter NSAID (she does not want to take anticonvulsants) and is addressing the herpes outbreaks with aciclovir in preparation for her wedding. With all these stressors it may be possible that emphasis is being placed on the psychosocial rather than the biomedical aspects of pain management in this case.
How should Ms AD be managed?
Commentary
Ms AD will require assessment and management across multiple domains. This is likely to involve multiple healthcare provider inputs, and co-ordination of this care will be important.
Diagnosis
A never-ending search for a biomedical diagnosis is generally unhelpful in patients with persistent pain, but serious pathologies and easily treatable conditions need to be excluded. Although the temporal course in this patient would suggest the pain is related in some way to the splash injury, it is possible that this is a coincidence or that the splash injury and associated events represent new stressors that have aggravated a mild pre-existing condition. In addition to a primary eye or orbital disorder, persisting facial/ocular pain should prompt consideration of headache disorders, trigeminal neuralgia, temporomandibular joint dysfunction, dental disorders and, rarely, intracranial pathology.
Evaluation of Ms AD should begin with a careful history of the pain, as this is diagnostic in many headache and facial pain disorders. The temporal course and associated symptoms will guide diagnoses around migraine and trigeminal autonomic cephalagias. Differing features of differential diagnoses for persistent temporal pain are listed in the Table.
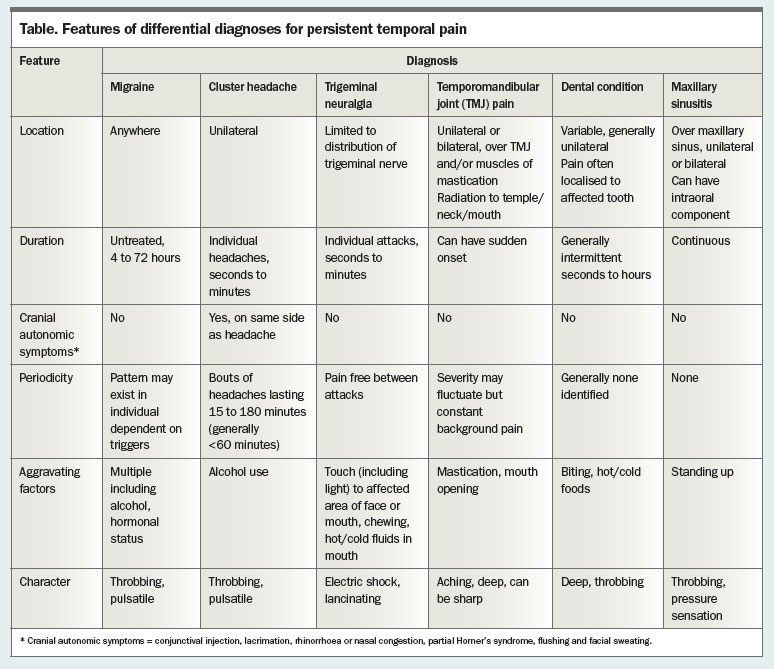{kind=link}
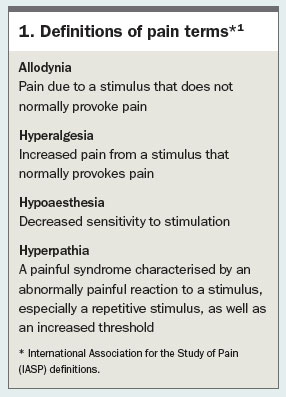
Examination should seek to identify any serious abnormality (ophthalmological assessment, neurological examination) as well as identify the presence and distribution of any sensory signs (allodynia, hyperalgesia, hypoaesthesia, hyperpathia; Box 1).1 The presence of hyperalgesia, hyperpathia and allodynia may point to central sensitisation.
{kind=link}
There may be no further need for investigations, although if trigeminal neuralgia is suspected consultation with a neurologist and an MRI of the brain and spinal cord should be considered to exclude multiple sclerosis as well as to assess for a vascular cause. The skin lesions should also be examined to confirm that they do not represent shingles.
The correlation between nervous system sensitisation and immune system imbalance is often observed. Stress can contribute to both conditions.
Psychological factors
Regardless of the cause of this young woman’s pain, the case illustrates the importance of considering psychosocial factors alongside the biomedical concerns of diagnosis and treatment. The patient has a fear of severe illness and there are also significant stress-related factors (mouth ulcers, concurrent wedding planning, the possibility of pregnancy or planning a pregnancy) as well as loss of employment (with its financial, identity and social implications/costs) and unclear comprehension of the importance of psychological factors.
It is worth asking Ms AD what she is most fearful of in relation to the pain. Identifying any specific fear opens the way for targeted reassurance. Asking about any other unusual or stressful events in the lead up to the onset of pain is worthwhile. There may be other factors beyond the eye splash and the wedding that need to be taken into account. In addition, Ms AD will benefit from identification and treatment of any comorbid psychological or psychiatric conditions (depression, anxiety and sleep disturbance being the most common). There may be pain catastrophising occurring, as evidenced by her worry about something ‘nasty going on’. This could be assessed using the Pain Catastrophising Scale, and potentially addressed with pain education with or without psychologist intervention.2
It will also be useful to assess what insight this patient has into the psychological factors that influence pain experience. Her training in psychology may or may not equate to personal insight. This in turn may influence her willingness to seek psychological input. It is also worth considering her skills in problem solving and whether these can be enhanced to help her deal with her circumstances.
Management options
Physical treatments
The specific physical treatments to be considered will depend on the diagnosis. In this patient, physical treatments may play a role in temporomandibular joint disorder (e.g. splints provided by a dentist to protect teeth), neuropathic pain (desensitisation for allodynia) and some headache disorders.3,4
Maintenance of general physical activity is advisable because of its general benefits on mood and pain. Staged increases in activity, particularly any activity associated with pain, can be used as a means of nervous system retraining.
Psychological treatments
Targeted reassurance can be directed towards any specific fears identified. Pain education can be facilitated by online resources such as the Pain Management Network (www.aci.health.nsw.gov.au/ chronic-pain), books and pain education sessions provided through pain management services (Box 2). The importance of nervous system sensitisation as a mechanism for persistent pain may need to be regularly reinforced and supported with the idea that this does not mean the pain is ‘made up’ or lacks treatment options.5
Formal psychological treatment may be considered, such as cognitive behavioural therapy or acceptance and commitment therapy strategies for specific pain complaints, and also techniques around goal setting and problem solving.6,7 Mindfulness-based therapies have received much attention recently and there is evidence to support their use in persistent pain and related symptoms such as anxiety.7 Patients with difficulty accessing psychology or pain management services because of, for example, location or cost may benefit from online treatment programs.
{kind=link}
Procedural options
Procedural options for management depend on whether any biomedical diagnosis is made. The full scope of possibilities is too broad to consider here, but diagnostic use of local anaesthetic blocks can identify contributing structures. There is a risk that overemphasis on procedural intervention can distract the patient from active engagement in physical and psychosocial approaches.
Pharmacological treatments
Regardless of what (if any) drugs are used for pain relief, it is key that the prescriber and patient understand that the goal is functional improvement rather than simply a reduction in pain scores. A global assessment measure (e.g. the Brief Pain Inventory) should be used to determine response to treatment.
A trial of simple analgesics is appropriate, but there should be a defined time frame, an appropriate dose (i.e. one that is expected to be therapeutic), a plan to re-evaluate and appropriate cautioning about risks (particularly with excessive dosing).
Several agents can be considered to address neuropathic pain and central sensitisation.8 If Ms AD’s pain is identified as neuropathic then tricyclic antidepressants (e.g. nortriptyline or amitriptyline starting at 5 to 10 mg at night and slowly titrating up to 25 to 75 mg) are appropriate first-line therapy with the best number needed to treat for neuropathic pain. Serotonin and noradrenaline reuptake inhibitors can be particularly helpful in addressing neuropathic pain concurrently with depression or anxiety as they are effective for both conditions. Use of anticonvulsants such as pregabalin or gabapentin may be a challenge in young people, who can find their adverse effect of cognitive impairment debilitating. A discrete area of neuropathic pain may respond to topical lignocaine (a 5% transdermal patch formulation is available but not PBS subsidised). Opioids are unlikely to have a role in treating neuropathic pain because of their long-term risks, including overdose, abuse and other harms.9
Should Ms AD be found to have a headache disorder then different agents are likely to be appropriate for treatment or prophylaxis of specific conditions.
A diagnosis of trigeminal neuralgia would suggest carbamazepine as first-line therapy.8
Care co-ordination
Care co-ordination will be a key role for the GP in Ms AD’s case. Ensuring that appropriate medical and allied health input occurs, balancing the role of medical specialist input against the potential for overmedicalisation of the situation, and encouraging a return to normal function while promoting the development of insight into her psychological state can all occur within this role.
Return to work
The benefits of return to work extend beyond the financial aspects and return to work is an important treatment goal for people with persistent pain.10 Work presents people with independence, a positive identity, social contact, satisfaction and structure. Ability to return to work in the context of pain is influenced by the beliefs and attitudes of the employee and employer, rather than by pain or any success of symptomatic interventions.11 Return to work is more likely when a short duration of time off work occurs and a return to work co-ordinator is involved.12
Failure to return to work at this stage may deny Ms AD the benefits of future work. The longer she does not work, the more likely she is to not succeed in subsequent attempts at employment. It would be important to establish whether the goal is to return to the previous job (her resignation is clearly a potential problem here) or to seek new employment. It would also likely be important to address the fear of a similar incident occurring, as well as her beliefs about how much the pain impacts her abilities. The general principles of return to work apply: a supported and staged return to work with progressive reintroduction of problematic duties (in this case, instrument cleaning). Assistance for this may be available through the appropriate Workcover insurers.
A comment on age
Age is an interesting factor in this case. Management plans need to consider that Ms AD may well have more than 50 years of life ahead of her. She may intend a pregnancy in the near future, thus there are implications for pharmacological treatment. Diagnostically, trigeminal neuralgia (and the associated possibility of multiple sclerosis) should be considered as a cause of the facial pain in a young woman. The exercise of successfully addressing psychosocial factors at a relatively young age can help build the insight and skills needed for lifelong wellbeing.
An appropriate outcome
A successful return to employment, regardless of whether pain persists, would be a satisfying outcome for this woman, her family, her treating team and society.PMT
References
- International Association for the Study of Pain(IASP) Taxonomy Working Group. Pain terms: a currentlist with definitions and notes on usage. In: Merskey H, Bogduk N, eds. Classification of chronic pain. 2nd ed. Seattle: IASP Press; 1994 (revised 2011). Available online at: http://www.iasp-pain.org/files/Content/ContentFolders/Publications2/ClassificationofChronicPain/Part_III-PainTerms.pdf (accessed April 2017).
- Sullivan MJL, Bishop S, Pivik J. The Pain Catastrophizing Scale: development and validation. Psychol Assess 1995; 7: 524-532.
- Ebrahim S, Montoya L, Busse JW, Carrasco-Labra A, Guyatt GH; Medically Unexplained Syndromes Research Group. The effectiveness of splint therapy in patients with temporomandibular disorders: a systematic review and meta-analysis.
- J Am Dent Assoc 2012; 143: 847-857.
- Racicki S, Gerwin S, Diclaudio S, Reinmann S, Donaldson M. Conservative physical therapy management for the treatment of cervicogenic headache: a systematic review. J Man Manip Ther 2013; 21: 113-124.
- Moseley Gl, Butler DS. Fifteen years of explaining pain: the past, present, and future. J Pain 2015; 16: 807-813.
- Eccleston C, Morley SJ, Williams AC. Psychological approaches to chronic pain management: evidence and challenges. Br J Anaesth 2013; 111: 59-63.
- Veehof MM, Trompetter HR, Bohlmeijer ET, Schreurs KM. Acceptance- and mindfulness-based interventions for the treatment of chronic pain: a meta-analytic review. Cogn Behav Ther 2016; 45: 5-31.
- Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: systematic review, meta-analysis and updated NeuPSIG recommendations. Lancet Neurol 2015; 14: 162-173.
- Chou R, Turner JA, Devine EB, et al. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann Intern Med 2015; 162: 276-286.
- Sullivan MJL, Hyman MH. Return to work as a treatment objective for patients with chronic pain?
- J Pain Relief 2014; 3: 130. doi: 10.4172/2167-0846.1000130.
- Nicholas MK, Linton SJ, Watson PJ, Main CJ; ‘Decade of the Flags’ Working Group. Early identification and management of psychological risk factors (‘yellow flags’) in patients with low back pain: a reappraisal. Phys Ther 2011; 91: 737-753.
- Hamer H, Ghandi R, Wong S, Mahomed NN. Predicting return to work following treatment of chronic pain disorder. Occup Med (Lond) 2013; 63: 253-259.
COMPETING INTERESTS: None.