Managing pain in cancer survivors

Cancer pain
Pain
Chronic pain can be caused by the side effects and complications of cancer treatment. An individualised, patient-based approach to pain management is important in cancer survivors and needs to take into account the pain mechanism, underlying cancer diagnosis, oncological treatments received, risk of recurrence, presence of comorbidities and performance status of the patient.
- Although people with cancer may experience chronic noncancer pain caused by comorbid conditions, chronic pain may also be caused from cancer treatment.
- Better management of pain caused by cancer treatment helps patients to complete therapy and improves cancer outcomes.
- All cancer treatment modalities can cause chronic pain, with postsurgical pain syndromes and chemotherapy neuropathy being the most common.
- Cancer survivors will benefi t most from a biopsychosocial approach to pain assessment and management.
- Chronic pain after cancer treatment should be managed in a similar way to chronic noncancer pain.
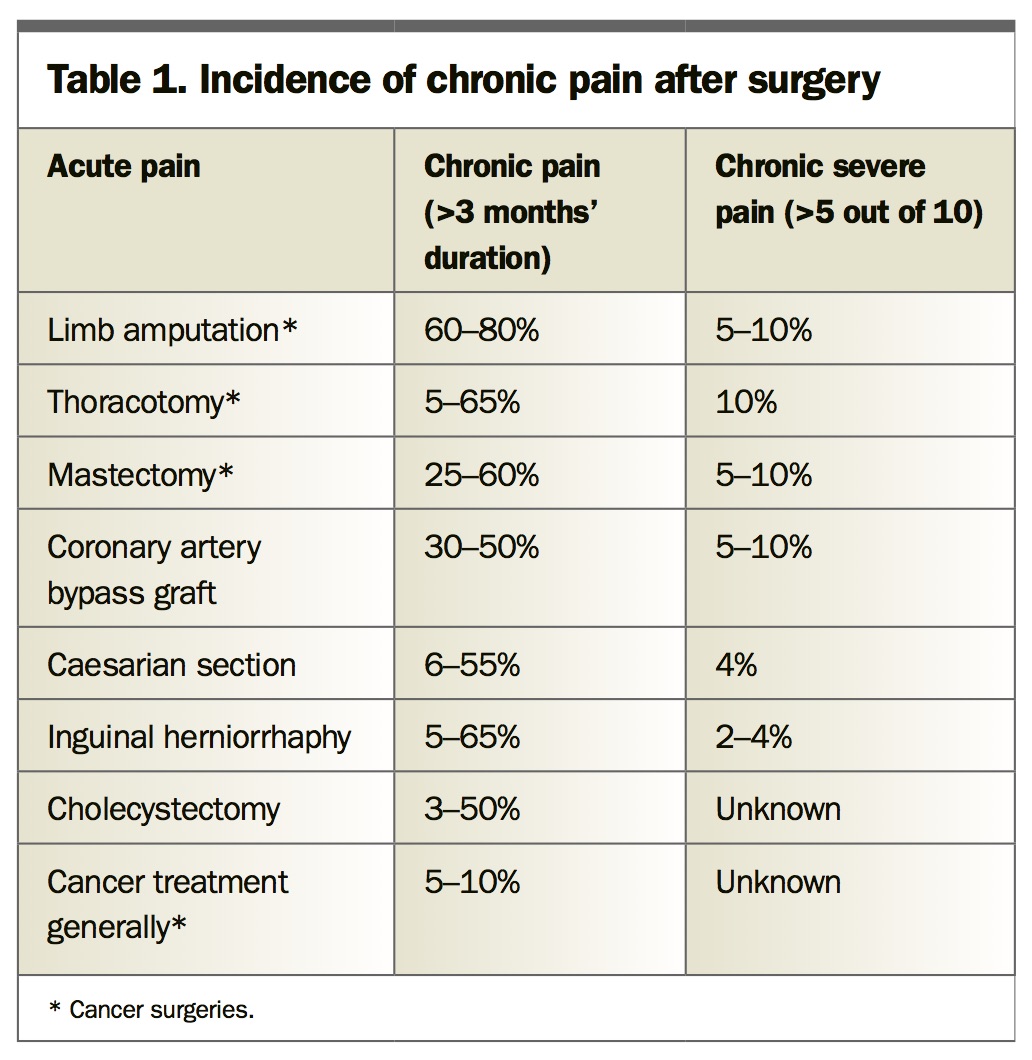
The five- and 10-year survival rates have improved substantially in people with cancer in the past three decades. Almost two-thirds of patients diagnosed with cancer can now expect to be alive in five years’ time. This improvement in cancer outcomes is attributable to a combination of screening and early diagnosis, more effective treatments and better supportive care. However, cancer treatment can cause pain, and it is estimated that about 40% of cancer survivors experience pain. Pain management, which allows patients to stay on course with their cancer treatment, is included in the supportive care advances. Fortunately, most acute pain caused by cancer treatment usually improves quickly, but it may become chronic (i.e. persist beyond the usual time needed for tissue healing, which is arbitrarily defined as 12 weeks by the International Association for the Study of Pain) in a small percentage of patients. Why acute pain becomes chronic and in whom depends on a variety of factors, including the type of surgery undertaken (Table 1), demographics, comorbidities and genetics.1
{kind=link}
The definition of a cancer survivor and the type of chronic pain need clarification when considering chronic pain in cancer survivors. According to the NSW Cancer Institute, cancer survivorship begins at diagnosis and includes people who continue to have treatment to reduce risk of recurrence or to manage chronic disease. It also includes the longer-term impacts of cancer treatment on people with cancer. Regarding the type of pain, it is noteworthy that chronic pain is common in the community (affects 20% of the Australian population and up to one-third of people over 65 years);2 therefore, chronic pain in many cancer survivors will be attributable to other problems (e.g. spondylosis, osteoarthritis, peripheral neuropathies). In one survey of American patients undergoing outpatient chemotherapy, almost half of them attributed at least some of their pain to causes other than the cancer or its treatment.3 This article focuses on the assessment and management of persistent pain attributed to a complication or side effect of cancer treatment.
Chronic pain syndromes from cancer treatment
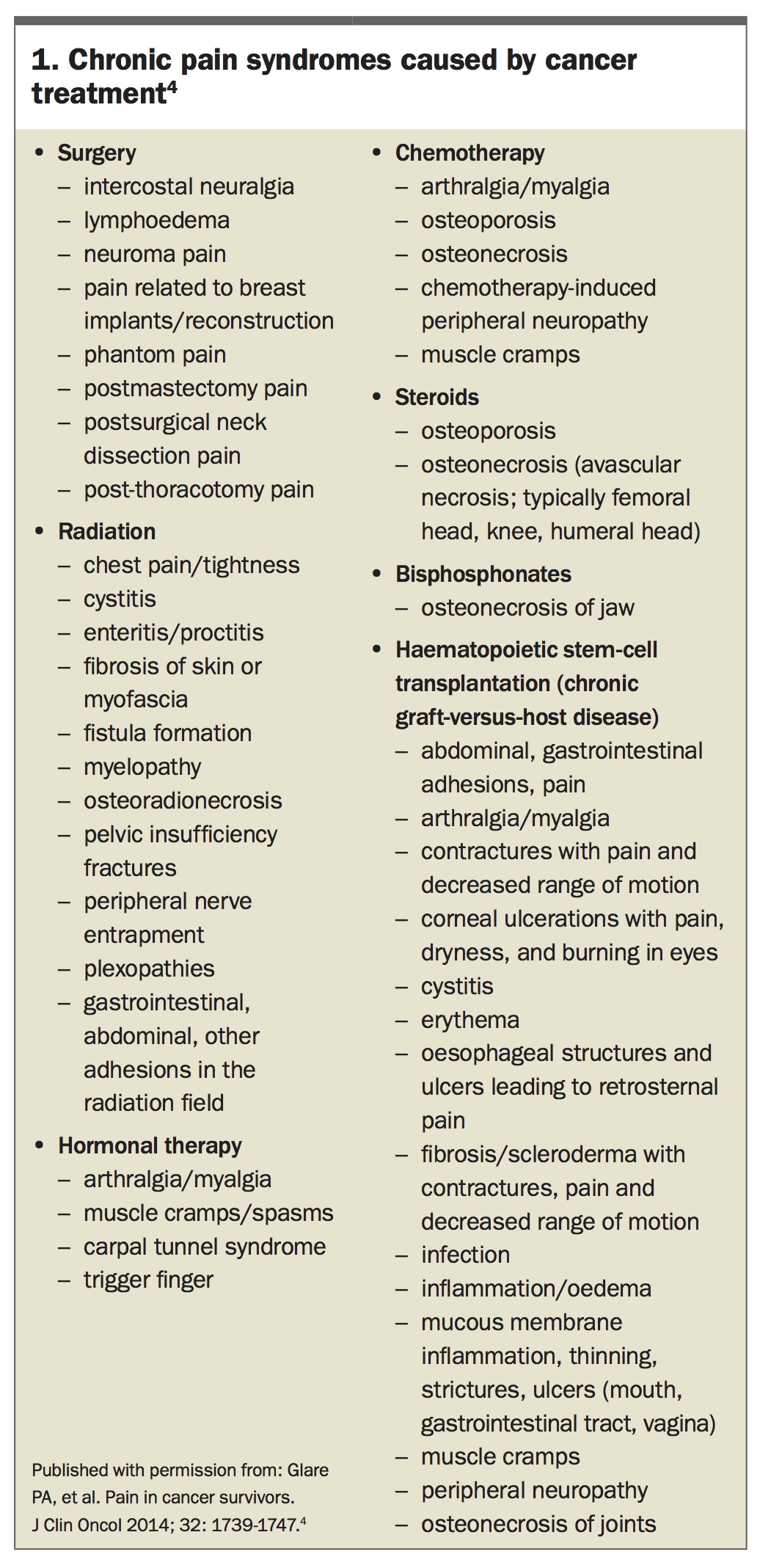
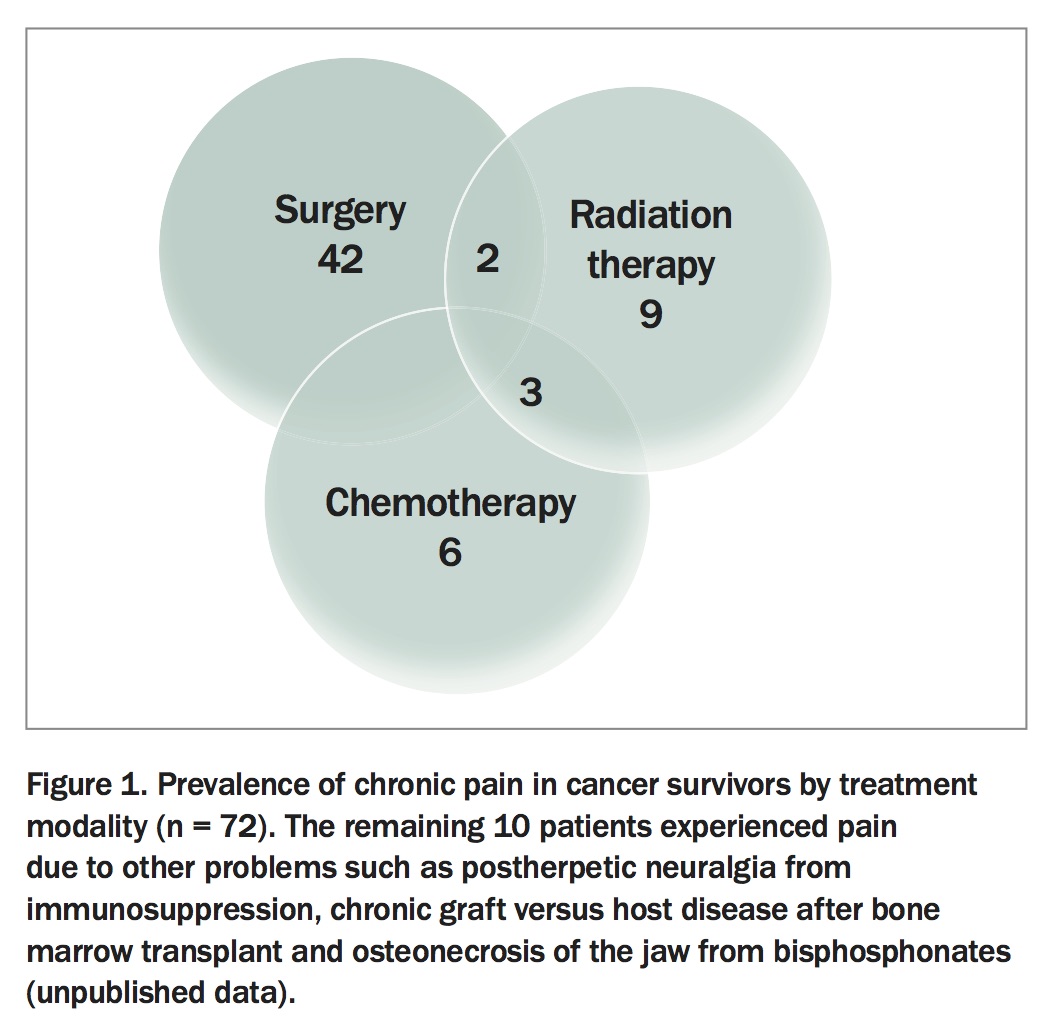
Many chronic pain syndromes may be caused by cancer treatment and these are listed in Box 1.4 The prevalence of chronic pain caused by different cancer treatments in 72 cancer survivors (average age 69 years and five years postdiagnosis) at Royal North Shore Hospital, Sydney, is shown in Figure 1. As cancer treatment is often multimodal, more than one treatment type can cause pain (e.g. mucositis from combination chemoradiotherapy). Postherpetic neuralgia and graft versus host disease are common in immunocompromised patients.
{kind=link}
{kind=link}
Persistent pain after breast cancer surgery
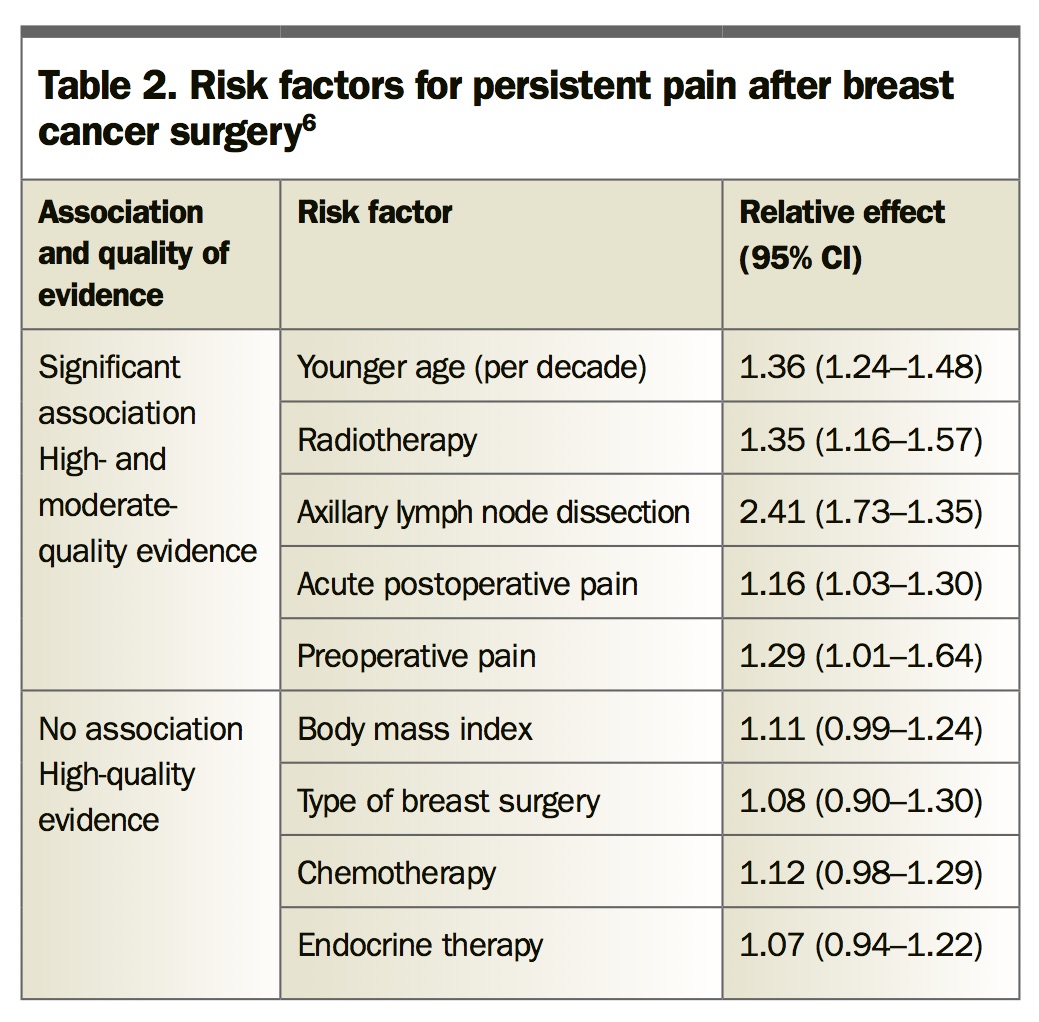
The most common and well-described pain syndrome in cancer survivors is postmastectomy pain, also known as persistent pain postbreast cancer surgery. More than 30% of patients report above-average pain 10 years after breast cancer surgery.5 Various predisposing factors have been identified (Table 2).6,7 There are multiple sources of potential tissue damage after breast surgery, including:
{kind=link}
- phantom breast pain (akin to phantom limb pain)
- secondary musculoskeletal pain (after mastectomy in women with large breasts)
- intercostobrachial neuropathy following lumpectomy with axillary lymph node dissection
- reconstruction surgery (transverse rectus abdominus myocutaneous flap; insertion of expanders)
- revision surgery.
General surgical factors increasing the risk of developing persistent pain postbreast cancer surgery include use of surgical drains, division or prolonged retraction of nerves and duration of surgery greater than three hours.8 Psychological factors may also be relevant, with studies indicating anxiety, depression, catastrophisation and somatisation were predictive of developing persistent pain postbreast cancer surgery,9 whereas ‘psychological robustness’ was protective.10
Chemotherapy-induced peripheral neuropathy
Many antineoplastic agents are neurotoxic, with oxaliplatin (used in bowel cancer) and paclitaxel (used in breast cancer and ovarian cancer) being the most commonly used neurotoxic agents. Some myeloma treatments are also neurotoxic. The development of chemotherapy-induced peripheral neuropathy (CIPN) is influenced by several factors, including the chemotherapeutic agent used and their cumulative dose, pre-existing nerve damage and presence of comorbidities (e.g. diabetes). Chemotherapy can be toxic in any part of the nervous system, but a distal, ‘glove and stocking’ sensory neuropathy is most common. Patients most often complain of numbness and tingling, imbalance and loss of manual dexterity. Dysaesthesias and paraesthesias can be intense enough to be described as pain. Autonomic dysfunction may also occur, especially with use of the agents vincristine and bortezomib. The effects of CIPN are often severe enough to make dose adjustment or cessation of treatment necessary, resulting in potentially suboptimal therapy. However, the cessation of chemotherapy does not guarantee resolution of symptoms. Symptoms may progress, or even first appear, after treatment cessation.8 Three months after completing treatment with these agents, 60% of patients still complain of CIPN.11
Radiation-induced pain
Radiation can damage nearby structures including nerve plexuses and the gastrointestinal tract and can lead to chronic pain. For example, abdominopelvic visceral pain associated with late radiation toxicity of treatment for cervical cancer is particularly challenging as it is often coupled with significant physiological and functional derangement (e.g. chronic diarrhoea) and psychological distress. Although opioids are antidiarrheal, care needs to be taken not to aggravate the situation by causing opioid-induced constipation.
Treatment of pain in cancer survivors
An individualised, patient-based approach to pain management is important in cancer survivors. The pain management plan needs to take into account many factors, including:
- pain mechanism (often neuropathic)
- underlying cancer diagnosis and oncological treatments received
- risk of recurrence
- presence of relevant comorbidities (e.g. renal impairment, mental health)
- performance status of the patient.
A biopsychosocial approach is most likely to be effective in cancer survivors, focusing not only on the mechanisms of pain but also on the physical, emotional and social consequences of chronic pain and how the patient is coping with it. Enlisting community resources such as physiotherapy and psychological support may be sufficient for patients with mild-to-moderate distress and disability but those with excessive problems are most likely to need referral to a multidisciplinary pain clinic.
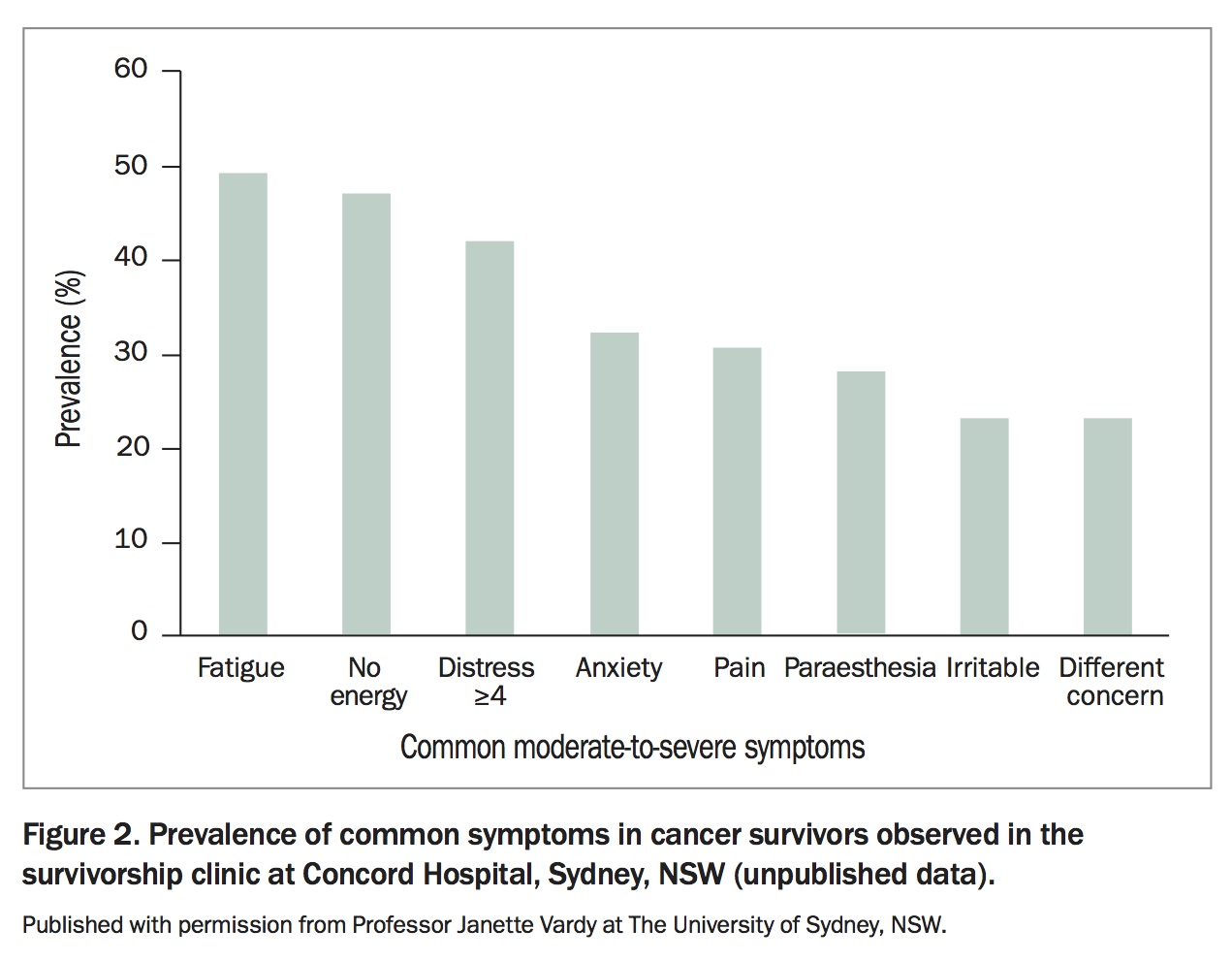
Pain rarely occurs in isolation, and survivors often have many other troublesome symptoms concurrently (Figure 2). In one survey, more than 90% of patients reported symptoms related to their cancer and/or its treatment at one year after diagnosis, with approximately one-quarter being in the ‘high symptom burden' category.12 Pain, depression and fatigue had the greatest impact on their quality of life. Anxiety, depression, fatigue and insomnia can exacerbate pain, and optimal management addresses all of these together.
{kind=link}
Treatment of persistent pain after cancer surgery
Pain after cancer surgery may be amenable to the same preventive strategies and combination treatments as for other postsurgical pain. These include the use of pre-emptive and protective analgesia using drugs such as gabapentinoids or antidepressants, which may reduce the development of neuropathic pain. Pre- and intraoperatively, local anesthetic infiltration and regional anaesthesia, such as paravertebral blocks, may be of some merit.13 In the postoperative period, it is important to maintain good analgesia; thoracic epidural analgesia can be especially effective following thoracotomy or upper gastrointestinal cancer surgery. Neuropathic pain should be identified early and treated effectively. Given the possible role of psychological factors in the development of persistent pain postbreast cancer surgery, psychological interventions and pain education during the perioperative period may also be beneficial.
Although opioids remain the mainstay of systemic analgesia for the treatment of moderate-to-severe acute pain,13 the emerging concept of oncoanaesthesia, in which anaesthetists use targeted therapeutic interventions in the perioperative period that may impact on patients’ cancer outcomes, is causing some uncertainty in this regard.14 Accumulating preclinical and epidemiological evidence indicates opioids may deleteriously impact on cancer survival via immunosuppression, increased angiogenesis, tumour growth and metastatic rate.15 Although this evidence remains preliminary, regional or neuraxial analgesia is proposed for reducing cancer recurrence in the perioperative setting, and this is in part attributed to their opioid-sparing effect.13
Treatment of peripheral neuropathy pain
Unfortunately, no agents have been proven to prevent the development of CIPN. In terms of treatment, duloxetine 30 to 60 mg/day has been shown to reduce pain intensity in patients with established CIPN compared with placebo.16 Trials of amitriptyline or gabapentin may also be considered, as they are efficacious in other peripheral neuropathies. Topical menthol cream has some efficacy in treating CIPN.17 Other topical pain preparations such as capsaicin 0.025% cream and 5% lignocaine patches can also be tried; although clinical trial evidence is lacking, their minimal adverse effect profiles make them popular options. They can also be tried in other cancer treatment-related neuropathies (e.g. postherpetic neuralgia in immunosuppressed patients). Nonpharmacological approaches are also advocated for treatment of other elements of CIPN, such as addressing psychological aspects and providing occupational therapy for adjustments and aids to assist with activities of daily living.
Role of opioids in cancer survivors
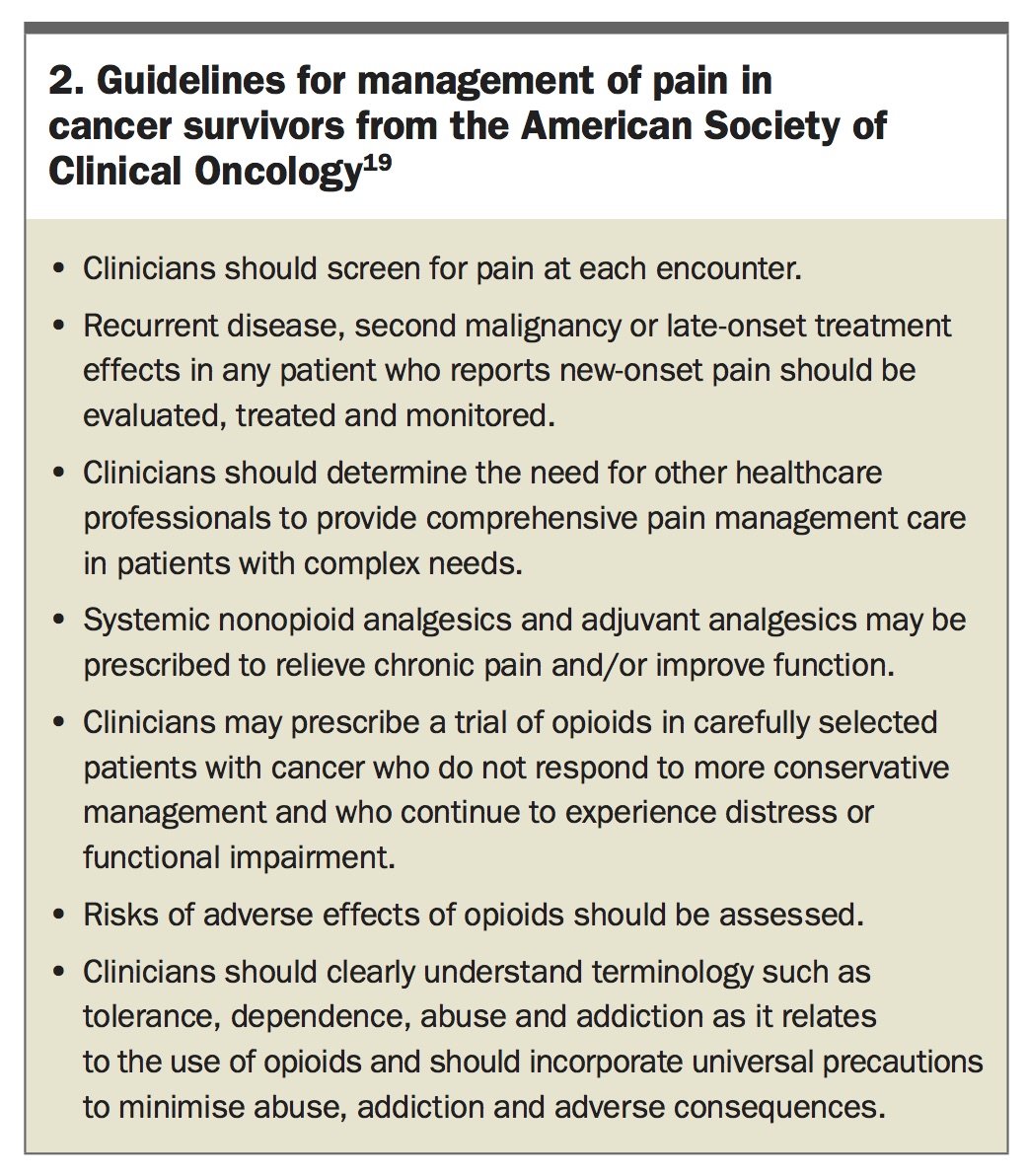
In our review of medical records at Royal North Shore Hospital, Sydney, 43% of cancer survivors were taking strong opioids at the time of their initial assessment – on average five years postdiagnosis – at a median dose of 83 mg oral morphine or equivalent per day. The role of opioids in cancer survivors is not straightforward. In the past, cancer treatment-related pain was considered as a subset of cancer pain,18 for which opioids are considered the mainstay of treatment. The American Society of Clinical Oncology guidelines on pain management in cancer survivors released in 2016 (in the early stages of awareness of the extent of the ‘opioid epidemic’) recommended that clinicians may prescribe a trial of opioids in carefully selected patients not responding to other measures and who continue to experience distress or functional impairment (Box 2).19
{kind=link}
Patients cured or in remission from cancer who have persistent pain are increasingly being seen as indistinguishable from people with chronic noncancer pain.8 The use of opioids in cancer survivors raises the same concerns and problems that challenge those treating patients with chronic noncancer pain. Not only are opioids ineffective for chronic noncancer pain, but the risks are increasingly being recognised, and 5 to 10% of patients will become addicted.18,20 The risk of dying within the next 2.5 years is 0.2%, and this risk doubles in patients also taking gabapentin.21 The risk of overdose from opioids in patients taking more than 50 mg oral morphine or equivalent per day is twice that of those taking less than 20 mg/day.7
If opioids are prescribed during cancer treatment, patients should be weaned as soon as possible in those with early stage cancer for whom cure is the goal. Some 5 to 10% of opioid-naïve patients become persistent users of opioids postsurgery, and patients with cancer are more likely to be in this group as they have many of the risk factors (e.g. thoracic surgery, major comorbidities [i.e. cancer], preoperative pain, smoking, alcohol/drug use, mood disorders).
Conclusion
Chronic pain can result from the side effects and complications of cancer treatment. Due to the benefits of screening and early diagnosis, many patients with cancer are completing definitive treatment for localised cancer with the prospect of long-term, disease-free survival, if not cure. If chronic pain develops, it should be managed in the same way as chronic noncancer pain, rather than a cancer pain. The aim should be to focus on treatment modalities other than long-term opioids, as chronic opioid therapy is ineffective and unsafe and better options are available. Chronic pain after cancer treatment needs the same biopsychosocial approach to assessment and management as other chronic pain. Patients with more severe disability and distress will benefit from referral to a multidisciplinary pain clinic. PMT