A practical checklist for managing chronic neck pain

Neck Injuries and Disorders
Pain
Long-term management of neck pain requires multimodal therapy similar to that for managing chronic low back pain. Psychosocial care and education are important options. Other treatments, particularly physiotherapy, are often directed at managing acute neck pain flare-ups.
- About 20% of people who sustain a painful acute neck injury will develop chronic neck pain over the following 12 months.
- Risk factors for developing chronic neck pain include severe acute neck pain, whiplash-associated disorder, psychosocial stressors, work factors, chronic headache, sleep disturbance, a sedentary lifestyle and smoking.
- Screening for red and yellow flags at every consultation is vital.
- Treatments are often directed at managing acute pain flare-ups.
- Most studies of physiotherapy treatments report only modest analgesic effects and improvements in function; however, there may be individuals who respond well to certain treatments.
- The checklist outlined in this article offers a practical clinical approach for managing neck pain in primary care; however, there is only limited evidence to support most of the treatments mentioned.
Chronic neck pain refers to pain lasting for more than three months in the posterior neck area, bounded by the occiput, C7 vertebra and anterior borders of the trapezii. Chronic neck pain may be associated with pain in the shoulders and interscapular zone, and in some cases with widespread body pain. Chronic headache (cervicogenic headache) and/or arm pain may be present in up to 20% of patients with chronic neck pain.1-3 The epidemiology, assessment and management of chronic neck pain parallels that of chronic low back pain.
Chronic neck pain affects 10% of adults at any given time and is more common in women, middle-age and higher socioeconomic and urban settings. Risk factors for developing chronic neck pain include severe acute neck pain, whiplash-associated disorder, psychosocial stressors (anxiety, post-traumatic stress disorder, depression), work factors (office-based work, manual labour, work dissatisfaction), chronic headache, sleep disturbance, a sedentary lifestyle and smoking.1-3 Chronic neck pain is a major cause of disability and economic burden, particularly after motor vehicle or workplace accidents.1-3
Given the significant personal and societal impacts associated with chronic neck pain, this article presents information and management strategies using a practical checklist approach that can be applied in primary care.
Causes of chronic neck pain
About 20% of people who sustain a painful acute neck injury will develop chronic neck pain over the following 12 months. Common inciting events for chronic neck pain include whiplash, postural loading (lifting, repetitive neck and arm movement, occupational overuse) and sports.1-3 Just as in chronic low back pain, a clear-cut ‘pain generator’ is not identified in 80% of cases of neck pain.
Where a musculoskeletal neck pain generator is identified, the most common sources are:
- facet joints (40% of cases)
- intervertebral discs (20% of cases)
- myofascial trigger points, particularly the trapezius.4
- Less common causes of neck pain include:
- spondylitis
- vertebral fractures
- vertebral end-plate (Modic) changes
- cervical plexus, spinal cord or sympathetic chain pathology
- vascular pathology (e.g. carotid or vertebral artery dissection)
- visceral pathology (i.e. thyroid, lymph glands, pharynx, oesophagus).
Red flag causes of chronic neck pain (Box) are rare, accounting for less than 5% of cases.
{kind=link}
Classification
The classification of neck pain is based on timing (acute or chronic), identification of a pain generator (specific or nonspecific) and the presence or absence of headache and/or arm pain. Most arm pain is ‘referred’ from musculoskeletal structures (e.g. facet joints, trigger points). Radicular arm pain is less frequent (10 to 20% of patients with arm pain) and commonly arises from the C5 or C6 nerve roots. The most frequent classification seen in primary care is chronic nonspecific neck pain.
Pathophysiology
The neck is vulnerable to injury such as whiplash and to physical loading such as occupational overuse. The neck contains numerous myofascial and neural structures that can generate pain. The head, neck and shoulder region is also susceptible to developing central (pain) sensitisation. Connections between the trigeminal nucleus (brainstem) and upper spinal cord (C2 to C4 levels) explain the strong link between neck pain and headaches.5,6 Interestingly, stress-related neck pain may reflect our quadruped ancestry, where increased muscle tension in the neck and shoulders allowed for escape from predators during ‘fight or flight’ situations.
Whiplash-associated neck pain
Whiplash-associated neck pain is a specific syndrome associated with flexion-extension loading of the neck, usually after a motor vehicle crash.1-3 Although in most cases whiplash does not cause structural damage in the neck, it may be associated with facet joint disruption (most frequently of the C5 or C6 joints), discopathy (annular tears), myofascial injury and less commonly, vertebral fracture, traction of the sympathetic chain in the neck or a cervical dural tear, which is associated with postural headaches.
Neck pain after whiplash may lead to injury compensation claims with impacts on work and finances, which can lead to stress, anxiety, catastrophising, depression and substance use (see yellow flags, Box). The best predictors for developing chronic neck pain and disability after whiplash are:
- onset of severe acute pain
- early neck disability
- psychosocial load (especially anxiety)
- evidence of pain sensitisation (allodynia) in the neck and shoulders.1-3
Multimodal pain management
Managing chronic neck pain is similar to managing chronic low back pain in that a multimodal, multidisciplinary approach is required. Treatments, particularly physiotherapy, are often directed at managing acute neck pain flare-ups in patients with chronic neck pain.
Prevention
There is some evidence that minimising whiplash and work- and sports-related neck injuries, and managing severe acute neck pain and psychosocial stressor load (yellow flags) may reduce the incidence of chronic neck pain and disability; however, further research is required in this area.1-3
Screening for red and yellow flags
Screening for red and yellow flag conditions at every consultation is crucial (Box). Red flags are rare but serious conditions causing pain, such as neurological deficits, fractures, metastatic cancer or infection, and should not be missed. An MRI scan of the cervical and upper-thoracic spine is the investigation of choice for most red-flag conditions. Yellow flags are psychosocial stressors associated with an increased risk of chronic pain and disability.
Physiotherapy management
Physiotherapy can be effective as part of a multidisciplinary pain management approach for the management of chronic neck pain and related disabilities.7-13 A physiotherapist is often the first professional to perform a comprehensive physical examination of the patient.
Physiotherapy management of chronic neck pain includes:
- comprehensive clinical assessment of the patient
- assessment of neck function and disability levels
- screening for red and yellow flags
- patient education
- managing patient expectations and concerns about their condition
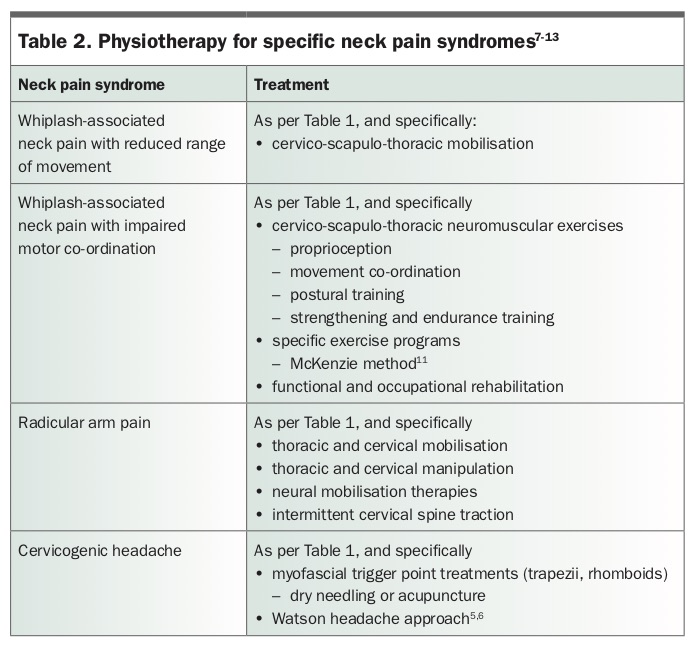
- applying evidence-based multimodal physical therapies (Table 1 and Table 2)
- managing associated pain conditions (e.g. headache, shoulder pain, interscapular spinal pain).
{kind=link}
{kind=link}
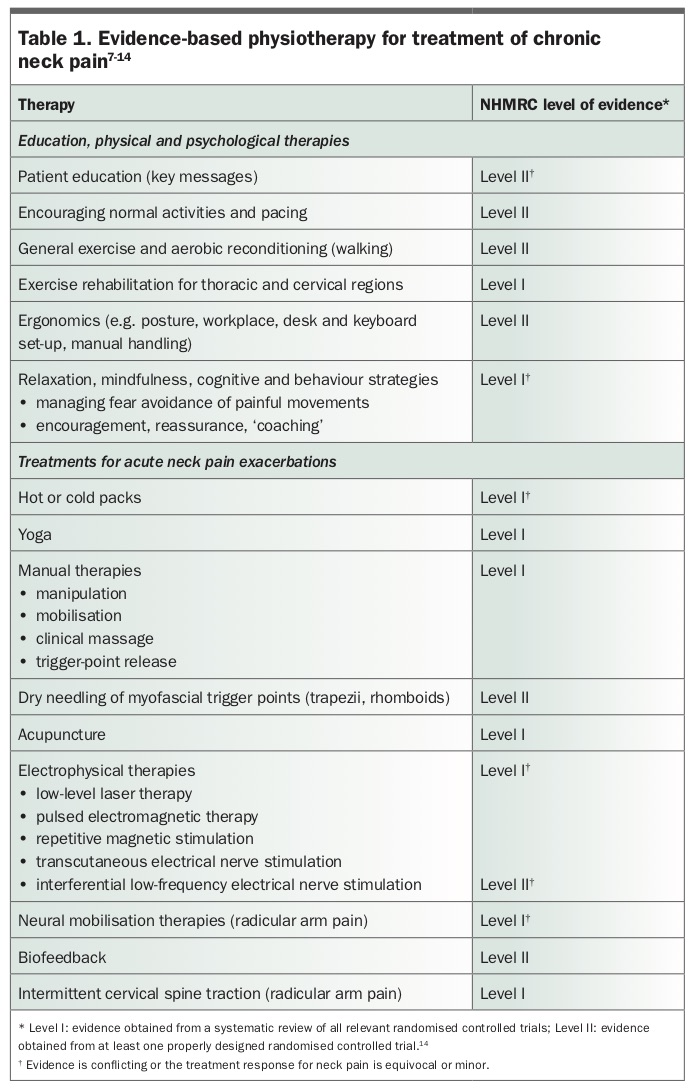
In agreement with recent international evidence-based guidelines, the 2002 Neck Pain Evidence-Based Clinical Statement of the Australian Physiotherapy Association recommended a multimodal physiotherapy approach to chronic neck pain, which is associated with improved strength, functional and pain outcomes.7,9 The 2017 American Physiotherapy Association evidence-based clinical practice guidelines for the management of chronic neck pain are summarised in Table 1.9
The effectiveness of any physiotherapy intervention requires ongoing reassessment to determine if it is the most appropriate treatment for a particular patient. Early referral to a physiotherapist and identification of factors that contribute to chronic pain are essential to preventing chronic neck pain. The risks versus benefits of each treatment must be considered by the therapist (e.g. the potential risks of cervical manipulation, traction, acupuncture or dry needling).
Evidence-based physiotherapy approaches for the treatment of chronic neck pain with NHMRC levels of evidence are listed in Table 1.7-14 For most treatments, evidence is of low-to-moderate quality and often conflicting. Most studies report an equivocal or minor analgesic effect for neck pain over a short period (usually days), with minimal improvement in function. However, following the tenets of personalised medicine, there may be individuals who respond well to certain treatments.
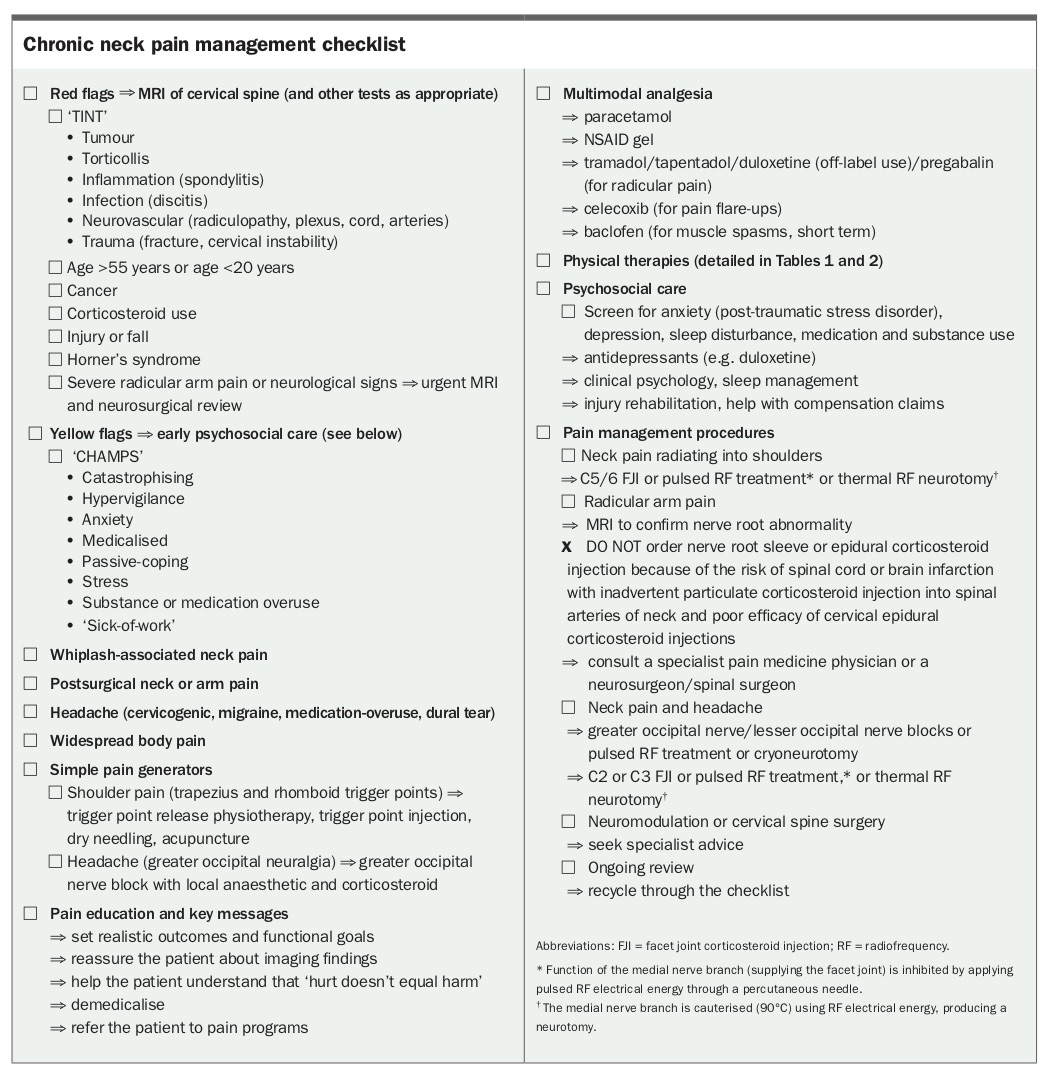
Medical management of chronic neck pain: a checklist approach
The checklist outlined in the Box offers a practical clinical approach for managing neck pain in primary care. However, there is only limited evidence to support most of the treatments mentioned.5-13
Conclusion
Chronic neck pain affects 10% of the population and is a leading cause of disability. The neck is vulnerable to injury and dysfunctional mechanical loading associated with whiplash, office or manual work and sports. The head and neck region is also susceptible to developing central (pain) sensitisation. Risk factors for transition to chronic neck pain after neck injury or postural or dynamic loading include severe acute pain, early impairment of neck function (disability) and increased psychosocial stressor load (yellow flags). Pain management requires a multimodal approach, including physiotherapy that is focused on patient education and restoration of neck function, and management of psychosocial load factors, particularly anxiety disorders. PMT
Acknowledgement
The authors acknowledge the contribution of Kimberley A. Zollner, physiotherapy student, Curtin University, Bentley, WA, to the writing of this article.