Chronic pelvic pain in women: the role of primary care

Chronic pelvic pain has multiple, intertwined aetiologies and is challenging to manage within short consultation times. General practice is often the starting point for evaluation of affected women and plays an important part in continuity of care and long-term follow up. Prompt management of dysmenorrhoea and dyspareunia may reduce the burden of chronic pelvic pain.
- Chronic pelvic pain (CPP) is a chronic or persistent pain perceived in structures related to the pelvis associated with negative cognitive, behavioural and sexual consequences in nonpregnant women lasting for more than six months.
- Women with CPP may also experience coexisting migraine or lower back pain.
- A comprehensive patient history is the most valuable tool in assessing a woman with CPP and is reliant on a strong patient–doctor relationship, coupled with regular follow up to overcome the barriers of time-limited general practice settings.
- Timely management of acute pain syndromes such as dysmenorrhoea or dyspareunia is achievable in primary practice settings, and provides important opportunities to prevent the development of CPP.
- Management approaches should prioritise improved function and general wellbeing over cure, with nonpharmacological approaches including physiotherapy intervention, psychological counselling and management of comorbidities as central components.
Picture credit: © Science Source/DNA Illustrations
Chronic pelvic pain (CPP) in women is a debilitating symptom of multiple, intertwined aetiologies. Despite an estimated global burden between 12.7% and 24%,1,2 CPP remains largely under-reported, poorly understood and may be challenging to manage within short consultation times. CPP is a chronic or persistent pain perceived in structures related to the pelvis associated with negative cognitive, behavioural and sexual consequences experienced by nonpregnant women lasting for more than six months.3 The inclusion of dysmenorrhoea or dyspareunia as components of this CPP definition is variable,4 but their significance as risk factors and early intervention opportunities should be acknowledged.2,3
Women with CPP account for 20% of all outpatient gynaecological referrals at an exorbitant cost to the secondary healthcare sector.2,5 However, general practice is often the initial starting point for evaluation of women with CPP, who often present with coexisting migraine or lower back pain. General practice also offers the benefit of continuity of care and most management options can be implemented without the need for specialist referral. Although chronic pain syndromes are estimated to cost Australia more than $6 billion annually in direct costs and significantly reduce the quality of life of affected women, CPP is not considered a national health priority area.6,7
GPs with an interest and skillset to manage CPP have the capacity to achieve substantial improvement in patients’ quality of life and act as a point of familiarity throughout the often lengthy, diagnostic process. Challenges in diagnosing and managing CPP lie in that it is rarely attributed to a single obvious pathology or source of tissue damage.1 Any combination of genitourinary, gastrointestinal, neurological, vascular or musculoskeletal system dysfunction may underlie the aetiology of CPP. In contrast to other chronic pain syndromes, CPP often has embarrassing gender, sexual and fertility overtones making the topic difficult to discuss and the doctor–patient interface even more crucial.8 The impact of CPP on sexual function is often particularly distressing and has significant impact on women’s personal relationships, self-esteem and willingness to openly discuss their symptoms. With high concurrent rates of depression, anxiety, somatic symptom disorder and childhood sexual abuse, the general practice environment further plays an important role in simultaneously managing these comorbidities, albeit over successive consultations and with multidisciplinary input.9,10
A retrospective study highlights the difficulty women with CPP have finding effective care, which showed that 28% of women (n = 5051) failed to receive a diagnosis for their CPP and only 40% had evidence of specialist referral within a four-year period.5 Interestingly, another study showed that only one-third of women with CPP seek advice from a healthcare professional, indicating that disease burden is largely underestimated.11 Although there are limited data exploring barriers to diagnosis and care, a multifaceted diagnostic and treatment approach beginning at the first point of care is essential.
Mechanisms of chronic pain and prevention opportunities
CPP results from a combination of nociceptive and neuropathic pain in variable degrees. Nociceptive pain is a consequence of actual or threatened damage to non-neural tissue via the activation of nociceptors,3,12 whereas neuropathic pain results from direct insult to the somatosensory nervous system and is typically described as a burning sensation or paraesthesia.1
Although there are clear intuitive and temporal distinctions between acute and chronic pain, a functional transition from one to the other is evident in clinical practice. Plasticity of the nociceptive system has long been implicated in this transition, but underlying mechanisms have only recently been uncovered. Hyperalgesic priming has been described in which transient inflammatory insults or environmental stressors trigger long-lasting hypersensitivity of nociceptors via activation of protein kinase Cε.12 Moreover, the role of both peripheral and central sensitisation in increasing receptor sensitivity through alteration of ion-gated channel activation kinetics and exaggerating pain response through summation of repeated, mild insults (wind-up) is largely acknowledged.13
In contrast to many other areas of chronic pain, it may be possible to recognise early and prevent CPP in women, as acute pain may trigger chronic pain syndromes and effective treatment can be instigated early.7 Dysmenorrhoea and dyspareunia have been identified as significant early risk factors for developing CPP.2 With more than 70% and 14% of women in Australia reporting dysmenorrhoea and dyspareunia, respectively, seizing early treatment opportunities at each general check up may significantly reduce the burden of CPP.
History taking and establishing the therapeutic relationship
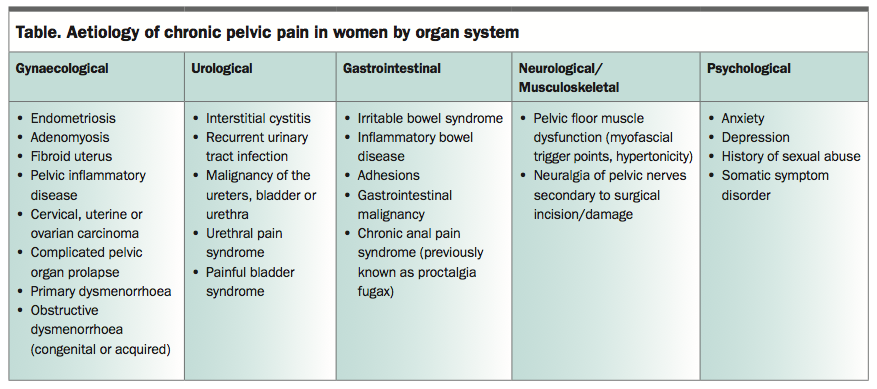
A comprehensive patient history is the most valuable tool in assessing a woman with CPP. Guidelines developed by the European Association of Urology promote a systems-based evaluation whereby the clinician evaluates each organ system and in the first instance excludes well known conditions associated with CPP such as endometriosis, painful bladder syndrome, irritable bowel syndrome or pelvic inflammatory disease (Table).14 Red flag symptoms such as rectal or vaginal bleeding, unintentional weight loss, altered bowel habits or abdominal bloating must be identified as abdominal or pelvic malignancies are rare but not uncommon, especially in postmenopausal women with CPP.
{kind=link}
Thorough scrutiny of the character of pain, duration, intensity, timing, exacerbations and relation to menses, sexual intercourse, defaecation, urination, recent surgery or childbirth should be elicited in the patient’s own words. This often provides a good indication of the causes of pain. The presence of multiple pain comorbidities is common. Overshadowing the patient’s description of their experiences with medical terminology negates a woman’s ability to take responsibility for her condition and strains the patient–doctor interface.15
Women with CPP want to be taken seriously, desire reassurance that their condition is not life-threatening and attach importance to having an explanation for their pain.15,16 A survey of women using CPP services in New Zealand reported an increasing loss of self-control with repeated doctor visits and lack of communication regarding investigation pathways and treatment options.15 The multifactorial nature of CPP should be openly addressed in early consultations and an assessment on restriction of daily activity made.4 Acknowledging the patient’s pain even in the absence of an obvious pathology is important, as is explaining that pain can persist long after a stimulus is removed. A patient questionnaire to assist GPs in taking a quick and comprehensive history is available from the Pelvic Pain Foundation of Australia website (www.pelvicpain.org.au/information/information-for-health-professionals/resources-women/), which can be completed confidentially.
Although difficult in busy practice settings, discussion of previous sexual, physical and emotional abuse should be included in any chronic pain assessment. Use of a questionnaire such as that provided by the Pelvic Pain Foundation of Australia may highlight this as a source of comorbidity and signal the need for psychological referral. Severe childhood sexual or physical abuse has been shown to be associated with a four- to six-fold increased risk of CPP in adulthood. 17 Furthermore, severe adolescent or adult sexual abuse was associated with greater CPP-related disability.10
Examination and investigation
Clinical examination of all abdominal and pelvic systems is an important step in the assessment of CPP but has limited specificity. However, focal tenderness, masses, distortion, engorgement and pelvic organ prolapse should be identified. Screening for both sexually transmitted diseases and urinary tract infections should be performed routinely. For women with risk factors for malignancy, measurement of CA-125 levels should be considered. Single digit palpation of at least the levator ani muscles should always be performed before speculum examination to assess pelvic floor tone and presence of myofascial trigger points.
Transvaginal ultrasound is useful in identifying adnexal masses and other relevant pathologies such as hydrosalpinx or fibroids. If transvaginal ultrasound is performed before laparoscopy, the presence of soft markers, such as tenderness or poor ovarian mobility, has shown to improve the likelihood of identifying relevant pathology at laparoscopy from 58 to 73%.4,17 Diagnostic laparoscopy remains the gold standard in the investigation of CPP as it is the only test that can reliably identify peritoneal endometriosis and adhesions, but its usefulness beyond this is limited. However, one-third to one-half of diagnostic laparoscopies will be negative in women with CPP and there are risks of serious complications such as adhesion formation, organ injury and/or perforation (2.4 in 1000) and death (1 in 10,000).4
Targeted treatment approaches
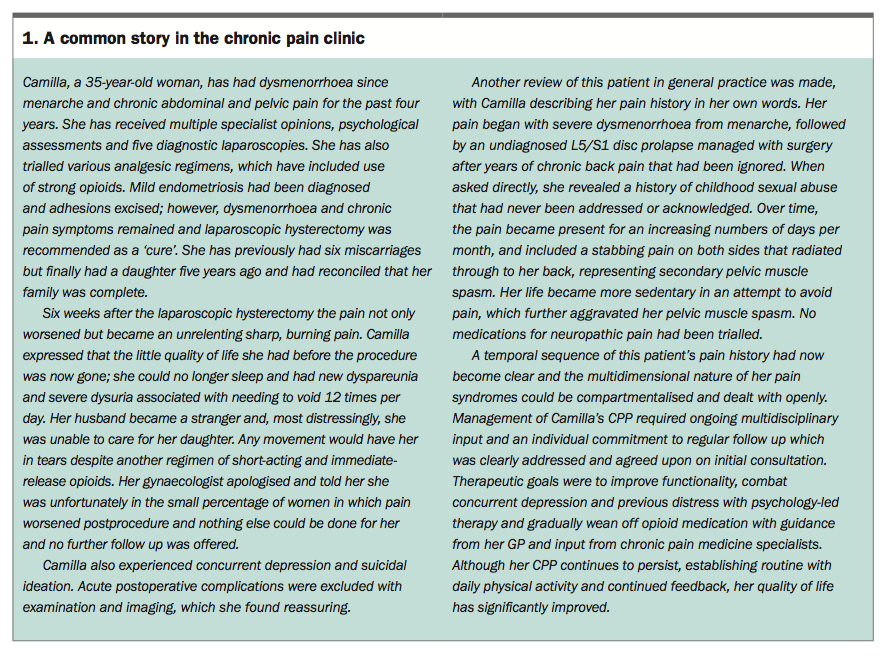
A story of a patient with CPP is described in Box 1 and serves as an important insight to the potential endpoints for a woman with CPP if not managed effectively in the early stages. Moreover, it highlights that a simple and holistic approach to pain instigated by a GP may curb unnecessary opioid use, allow for allied health assessment such as physiotherapy and provide continuity in long-term care. An approach to care that prioritises improved function and general wellbeing over cure is an emerging focus of CPP management, which must be tailored to the individual.7
{kind=link}
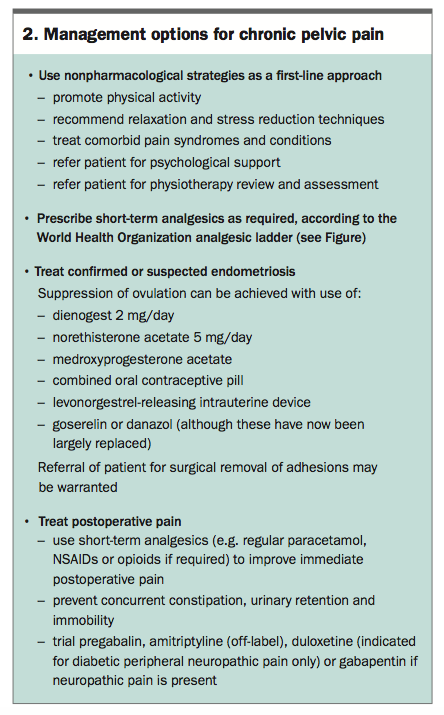
Although the development of CPP shares common beginnings with other pain syndromes, there are a few defined aetiologies that are implicated in CPP specifically and warrant additional treatment considerations (Box 2).
{kind=link}
Basic principles
Treatment of CPP should begin with nonpharmacological strategies. Although there is limited, high-grade evidence evaluating these strategies specifically to CPP, studies of other chronic pain syndromes provide basic principles that can be extrapolated and safely applied.
Promote regular physical activity
Regular, low- to moderate-intensity physical activity (aiming for 50 to 60% of maximum heart rate) increases physical function and has been shown to be slightly effective in reducing chronic lower back pain.18,19 Although avoidance of exercise in acute flares of pain is tempting, sedentary behaviour may worsen symptoms causing secondary spasm, and this should be discussed with patients. Low-intensity warm-water pool exercise performed twice per week was shown to have an immediate positive effect on pain in people with fibromyalgia20 and may be worth trialling as a gentle introduction to physical activity for women with CPP.
Treat comorbid pain syndromes and concurrent conditions
A prospective study of 108 women with CPP with or without endometriosis showed that 67% had a lifetime prevalence of also experiencing migraines.21 This not only contributes to the disability of CPP, but also highlights that both pain syndromes may share a common pathophysiology requiring consideration in the management of CPP.21 Lessons learned from clinical practice highlight that this may be true of other chronic pain syndromes coexisting with CPP. Minimising constipation, treating bladder pain and screening for urinary tract or sexually transmitted infections should also be considered.
Offer psychological support
As chronic pain is related to depression and anxiety, psychological support can provide women with valuable coping strategies and a safe place to address previous distress. A Cochrane review demonstrates that cognitive behavioural therapy offers some improvement in pain and a moderate benefit in pain-associated disability in patients with longstanding disabling pain, when compared with behavioural therapy or no treatment.22
The role of analgesics
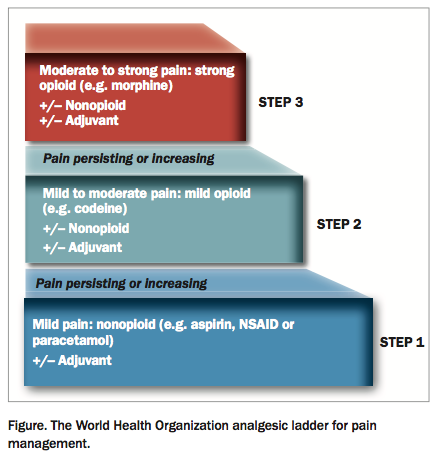
Use of the principles of the World Health Organization analgesic ladder is an important foundation for the treatment of acute and chronic nonmalignant pain, which can be instigated at all levels of health care (Figure).1 Focus should be placed on the synergistic action of nonpharmacological strategies with use of paracetamol, NSAIDs and milder opioids (e.g. tramadol or tapentadol) depending on underlying aetiologies. Stronger opioids such as oxycodone, morphine or methadone are best avoided because of their side-effect profiles and addictive properties. They are only appropriate for short-term use with guidance from pain specialists and should not constitute mainstay therapy.
{kind=link}
Treatment of dysmenorrhoea in women with endometriosis
It is estimated that between 70 and 90% of women with CPP also have endometriosis, although disease severity fails to correlate with pain severity.23 Menstrual suppression is the goal of symptomatic treatment and is readily achieved with use of the combined oral contraceptive pill, etonogestrel implant, medroxyprogesterone acetate or the levonorgestrel-releasing intrauterine device depending on patient preference and individual contraindications. Use of goserelin (a gonadotrophin-releasing hormone agonist) or danazol have been shown to reduce pain associated with endometriosis;4 however, use must be limited to six months and their respective side-effect profiles have ensured they are now largely replaced in clinical practice.
Recent attention has been placed on the use of low-dose progestins. Dienogest 2 mg per day has been shown to significantly reduce pelvic pain in women with endometriosis, and this effect lasted for at least 24 weeks after treatment cessation.24 However, one-quarter of women using dienogest still required simultaneous analgesic use.25 Long-term use of norethisterone acetate 5 mg per day is also an appropriate alternative, and comes with an added contraceptive effect.25 Irregular uterine bleeding, particularly in the first weeks of use, is a common side effect of all long-term progestogens and should be discussed before initiating treatment to improve long-term therapy compliance.24
Removal of mild to moderate adhesions of endometriosis via laparoscopic surgery was found to significantly improve CPP with no difference between excision or ablation techniques identified.26 Postoperative insertion of the levonorgestrel-releasing intrauterine device should also be considered, with significant reduction in the reoccurrence of dysmenorrhoea and greater patient satisfaction demonstrated when compared with no postoperative treatment.27
Management of pelvic muscle pain and dysfunction
Hypertonicity of the pelvic floor muscles is thought to develop from a vicious cycle of inflammatory, cognitive and behavioural factors that trigger a defence-to-pain response with overly tight and painful pelvic muscles. Pain is commonly stabbing and aggravated by prolonged positions, core-strength exercises or vaginal penetration. Myofascial pain is a regional condition characterised by the presence of myofascial trigger points across the levator muscles, which are focally taut bands within the muscles themselves.28
Failure to recognise dysfunction of pelvic floor muscles contributes to 24 to 40% of negative laparoscopy results.29 The importance of physiotherapy with pelvic floor muscle exercises, biofeedback and electrical stimulation techniques is well documented and early referral of the patient to a physiotherapist who is experienced in the management of tight and painful pelvic floor muscles is paramount.
Injection of focally tender points with a long-acting anaesthetic such as bupivacaine has had reported success,1 as has the use of botulinum toxin A (off-label use) for patients with refractory myofascial pain.30
Treatment of postsurgical pain
A positive correlation between a history of caesarean section and CPP (odds ratio 3.7; p<0.05) has been shown even when additional causes of pelvic pain were accounted for in a study of 199 Brazilian women.31 The incidence of nerve entrapment after one pfannenstiel incision is 3.7%.4 After an abdominal hysterectomy, the prevalence rate of pain varies from 5 to 32%.32 It is estimated that 10% of women experience significant pelvic pain up to three months after childbirth, and this is likely to be higher in the 35 to 40% of women who have episiotomies.33 Assessment of pain severity and effects on function should therefore be routinely discussed at postnatal checks.
Tissue injury postsurgery has both an inflammatory and neuropathic component related to direct damage to nerves traversing the surgical plane and can apply to any surgical intervention in the abdomen or pelvis.34 Antiepileptics (such as gabapentin and pregabalin), serotonin and noradrenaline reuptake inhibitors (such as duloxetine [indicated for diabetic peripheral neuropathic pain only]) and tricyclic antidepressants (such as amitriptyline [off-label use]) constitute the mainstay of neuropathic pain therapy. A reduction in neuropathic pain intensity by 50% has been shown in 35% of patients with chronic pain taking gabapentin, compared with 21% taking placebo.34 Although this study was not specifically in women with CPP, gabapentin may be reasonable to trial in these patients. Gabapentin with or without amitriptyline may be better for refractory neuropathic CPP than amitriptyline alone.16
Take home points to consider
CPP is common and often mismanaged within the constraints of a time-poor model of care. The presence of multiple pain symptoms and pain comorbidities is common and treatment may require trialling a range of options. A step-wise and thorough approach beginning with the patient’s story is fundamental to identifying the multiple components that have led to the patient’s pain experience. Importantly, early effective management of acute pain, including dysmenorrhoea or postsurgical pain, has the potential to prevent or minimise CPP.
With a focus on symptom support rather than cure, timely instigation of multidisciplinary management and open acknowledgment of this process, substantial improvement in quality of life for women with CPP can be achieved.PMT