Sciatica: how to assess it, what to say and when to worry

Sciatica
Sciatica is a common presentation in general practice, with pain often settling with conservative management. However, it is important to identify red flags and to understand the types of pain and pain generators that can give rise to sciatica.
- The term sciatica is often used to describe nonspecific back and leg pain; however, it is a confusing term and specific terminology to describe the pain should be used instead.
- Red flag conditions are not common in people with sciatica but need to be considered in all cases.
- Although imaging should not be routinely offered to people with sciatica and low back pain, MRI or radiography can be considered in certain clinical situations.
- Most cases of sciatica resolve within three months of conservative management.
- Referral of the patient to a specialist pain service should be considered if there is severe pain, the pain significantly limits their lifestyle or conservative therapies are ineffective.
Picture credit: © psdesign1/Adobe.com
Sciatica is often used to describe nonspecific back and leg pain, which is a common complaint that affects most people at some point during their lifespan. In many cases the pain settles with conservative management but it is important to identify red flags and have an understanding of the differing types of pain and pain generators that can give rise to sciatica. A safe and effective management plan will improve patient outcomes and satisfaction.
Anatomy of the sciatic nerve
The sciatic nerve, the longest nerve in the body, originates at the lumbosacral plexus, where the fourth and fifth lumbar nerve roots and the first two sacral nerve roots merge to form the sciatic nerve.1 The sciatic nerve leaves the pelvis through the greater sciatic foramen and descends in the medial aspect of the thigh down to the popliteal fossa where it divides into the peroneal (common fibular) and tibial nerves (Figure).
{kind=link}
What is sciatica?
The term sciatica is often used in a nonspecific manner to describe any back pain with radiation to the lower limb(s). It is a confusing term and means different things to different medical professionals and patients. Sciatic pain may be nociceptive, neuropathic or both. The term sciatica does not define aetiology or pathology. Sciatic pain usually originates at the nerve roots of the sciatic nerve but pathology (e.g. entrapment, inflammation, mass lesion) at any level along the course of the nerve can also lead to pain. Sciatica is also sometimes used as a synonym for radicular pain in the distribution of the sciatic nerve, which is neuropathic, typically with lancinating, shock-like electric qualities.2
Neuropathic pain
Neuropathic pain arises as a direct consequence of a lesion or disease affecting the somatosensory nervous system. This lesion or disease could affect the peripheral nervous system or the central nervous system. Pain descriptors include burning, tingling, electric shocks, pins and needles and numbness. The pain occurs within specific dermatomes correlating to the affected nerve(s). Neuropathic pain can occur at any time and can be independent of movement.
Nociceptive pain
Nociceptive pain might arise from the mechanical and bony aspects of the spinal column. It might also arise from the surrounding myofascial tissue. Pain descriptors include deep, aching and sharp, and usually the pain occurs in the back and surrounding area. Nociceptive pain is generally triggered by movement or is movement related.
Referred pain
Referred pain is defined as pain that is perceived at sites distant to the site of noxious or neuropathic stimulation and is thought to arise from neuronal convergence in the spinal cord. The referral pattern of neuropathic pain is typically neuropathic and the referral pattern of nociceptive pain is typically somatic.
Neuropathic referred pain is typically described as burning, tingling, electric shock, pins and needles, and paraesthesia in the distribution of a nerve or nerve root. Somatic referred pain occurs in a wider but local area around the pain generator (e.g. the L5/S1 facet joint can refer pain in a broad area that extends from the lower back to the buttock and upper posterior thigh). Somatic referred pain is generally described as a nociceptive pain and does not typically have neuropathic descriptors.
Radicular pain and radiculopathy
Radicular pain implies pain in a dermatomal distribution with no associated weakness, whereas radiculopathy displays weakness with other clinical features that may include atrophy, fasciculations, reduced reflexes and altered sensation. Pain is not necessarily a feature of radiculopathy. However, radiculopathy may coexist with radicular pain. A radicular syndrome is a term sometimes used when both radicular pain and radiculopathy coexist.
What are the causes of sciatica?
Sciatica may be caused by intraspinal or extraspinal factors anywhere along the course of the nerve, with intraspinal factors being the most common. A nerve root compression inside the spinal canal or the intervertebral foramen caused by a lumbar disc protrusion or prolapse is the most common intraspinal cause. In this situation, the most common affected areas are at the L4/L5 and L5/S1 levels. Disc protrusions cause up to 90% of cases of sciatica.3 Other causes of intraspinal nerve root compression include intervertebral foraminal stenosis caused by factors other than a protruding disc. These factors include facet joint arthropathy/hypertrophy, cyst formation and ligamentum flavum hypertrophy. A degenerate intervertebral disc loses height and this may result in a reduced diameter of the intervertebral foramen, thereby also causing foraminal stenosis.
Extraspinal causes may include spondylolisthesis (slipping of one vertebral body on another causing misalignment and narrowing of the intervertebral foramen), piriformis syndrome, trauma to the sciatic nerve (e.g. from an intramuscular injection in the buttock), direct trauma (such as from a fall) or compression of the sciatic nerve anywhere along its course (e.g. caused by a fracture, haematoma, tumour or infection). The sciatic nerve can be injured during surgery such as hip arthroplasty, although this is not common. Pain originating from the sciatic nerve de novo is also not very common.
Is there a better term than sciatica?
It is preferred to be precise and use specific terms when describing back and/or leg pain. The features of the pain and likely diagnosis should be described, rather than using a nondescript term such as sciatica. An example of describing the pain might be ‘there is radicular pain in the L5 dermatome distribution which is likely caused by a nerve root impingement at the L5 to S1 level’. Descriptors such as radicular pain for pain that occurs in a dermatomal distribution or radiculopathy if there are motor signs and weakness can be used.
Another issue with the term sciatica is that it does not imply any urgency for further investigation or therapy and it does not indicate if there are any associated red flags.
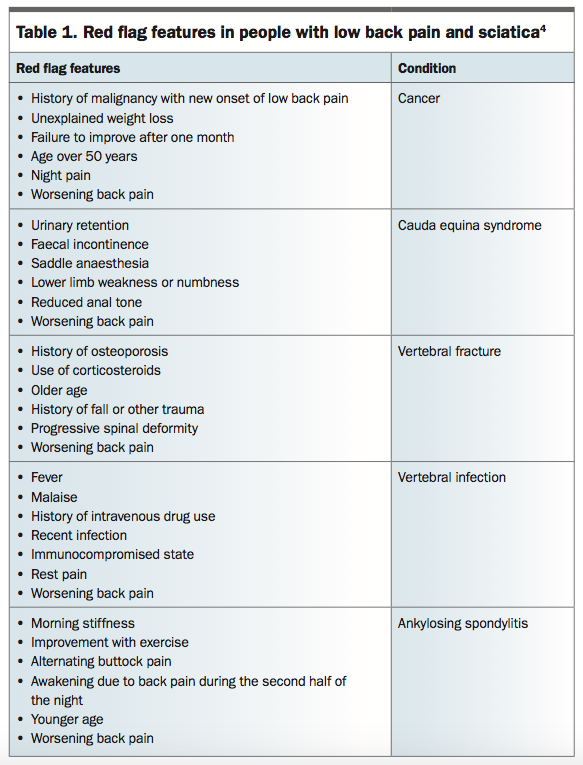
What are the red flags?
Red flag features, if present, should not be ignored (Table 1).4 Red flags are not common but need to be considered in all patients presenting with sciatica.4 Blood tests for investigation of red flag conditions may include myeloma screen, full blood count and measurement of erythrocyte sedimentation rate, C-reactive protein, urea and electrolytes and calcium levels.
{kind=link}
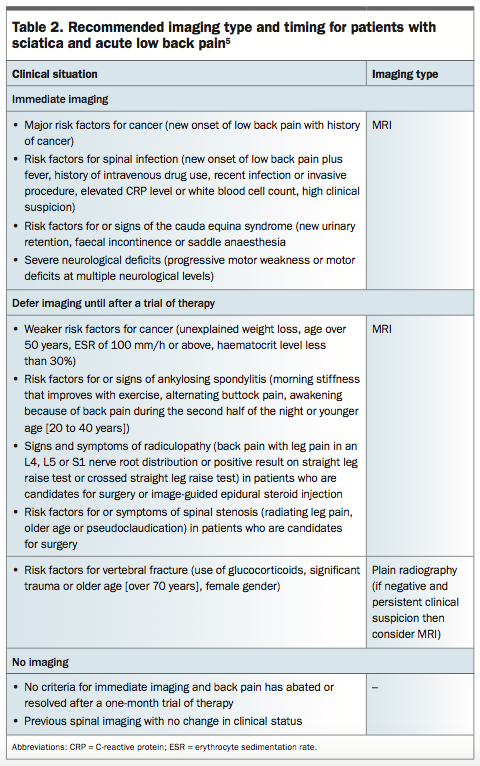
Imaging
Imaging in a nonspecialist setting for people with low back pain with or without sciatica should not be routinely offered. The recommended type and timing of imaging, if required, in different clinical situations in patients with sciatica and acute low back pain is outlined in Table 2.5
{kind=link}
Clinical points to consider in the assessment
Is there associated back pain?
If there is associated back pain, the differential diagnosis may broaden to include lumbar facet joint syndrome. If present, the signs may include unilateral/bilateral paraspinal pain with local radiation, pain on hyperextension and loading the facet joints, and pain on direct palpation of the facet joints.
Is there associated buttock pain?
If there is associated buttock pain, the differential diagnosis may broaden to include sacroiliac joint pathology. If present, symptoms include unilateral/bilateral pain in the upper buttock, pain worsening on loading the sacroiliac joint and reproduction of pain on direct palpation of the sacroiliac joint.
Piriformis syndrome should also be considered if there is associated buttock pain. If present, there may be pain radiating a varying degree down the sciatic nerve with possible pain on resisted hip abduction in the sitting position (Pace’s sign). Other signs of piriformis syndrome might include pain on flexion, abduction and internal rotation of the hip (positive FAIR test).6
Is there a dermatomal distribution of the pain?
A dermatomal distribution of the pain may provide a guide to the origin of the pain (e.g. an L5 radicular pain would include pain in the dorsum of the foot and big toe). An S1 radicular pain may include the sole and/or lateral aspect of the foot.
Is this a chronic pain condition?
Chronic pain is commonly triggered by an acute injury or disease but is then usually perpetuated by factors other than the cause of the pain. Perpetuating factors include stress and environmental and emotive factors. Pain should be considered to be chronic if the pain persists for more than one month after anticipated tissue healing or if pain continues for more than three months.
Chronic pain is considered pathological pain in that it is a maladaptive response to tissue inflammation or neurological damage and causes pain of no biological value.
Therapy for chronic pain should encompass the five pillars of multidisciplinary pain management, which include use of nonopioid medications, pain interventions if appropriate, physical therapy, functional therapy and psychological therapy.
Treatment of low back pain and sciatica
In most cases of sciatica the prognosis is good, with 75% of patients recovering within three months with conservative management.7
Noninvasive treatments
Nonpharmacological interventions
Nonpharmacological approaches for people with sciatica include self-management (providing reassurance, information and encouragement to keep moving their bodies), exercise (group program or manual therapies as part of a multidisciplinary approach), psychological therapy (cognitive behavioural therapy as part of the multidisciplinary approach), combined physical and psychological program, and promoting and facilitating return to normal activities and work.
Pharmacological interventions
Evidence-based pharmacological treatment of neuropathic and chronic pain includes use of high-dose gabapentinoids (gabapentin 1200 to 3600 mg/day in three divided doses, pregabalin 300 to 600 mg/day in two divided doses), serotonin and noradrenaline reuptake inhibitors (duloxetine up to 120 mg/day [indicated for diabetic peripheral neuropathic pain only], venlafaxine extended release 150 to 225 mg once a day [off-label use for neuropathic pain]), tricyclic antidepressants (amitriptyline or nortriptyline 25 to 150 mg/day [both off-label uses]).8-10
However, a recent study in 2017 found that pregabalin did not significantly reduce the intensity of leg pain or improve outcomes in people with sciatica compared with placebo, and was also associated with a higher rate of adverse events.11 This study demonstrates the complex nature of pain mechanisms in sciatica and that there is no one-size-fits-all approach. It should also be noted that high doses of medications are usually not tolerated by some patients especially the elderly or frail.
Oral NSAIDs should be used with caution, considering potential side effects and prescribing the lowest effective dose for the shortest time. Weak opioids such as tramadol can be considered for managing people with acute low back pain only if NSAIDs are not effective or are contraindicated. Opioids should not be routinely used for people with acute low back pain and should not be offered to those with chronic back pain. Furthermore, paracetamol alone should not be used for managing low back pain.8
Invasive treatments
Nonsurgical interventions
Radiofrequency denervation can be considered for people with chronic low back pain but should only be performed after a positive response to a diagnostic medial branch block.8 These people should be managed by appropriately trained medical specialists (e.g. interventional pain specialists) who can adequately assess and manage facet-mediated pain using diagnostic medial branch blocks.
Epidural injections of local anaesthetic and steroids can be considered in people with acute and severe sciatica.8 In the acute or subacute setting in which isolated lumbar nerve root irritation is clearly suspected, transforaminal nerve root blocks can provide useful diagnostic information as well as deliver targeted steroid treatment.12 Targeted nerve root injections should be considered rather than generic and nontarget-specific midline epidural injection, although sustained pain relief can be achieved with both types of epidural injection.
Surgical interventions
If red flag conditions have been diagnosed, a surgical opinion will usually be considered. Surgery per se has a limited role in the management of low back pain.
Spinal decompression for people with sciatica should be considered if nonsurgical treatment has not reduced pain or improved function and radiological findings are consistent with sciatic symptoms. It is difficult to define how long conservative therapy should be offered for but usually two to three months would be considered usual practice. Patients should be reviewed often and if their pain or symptoms worsen or change, a surgical opinion might be considered earlier.
For patients with degenerative disc disease with presumed discogenic back pain, the surgical options include microdiscectomy, spinal fusion and artificial disc replacement; however, it has been noted that spinal fusion is no more effective than interdisciplinary rehabilitation.13,14 The recent 2016 National Institute for Health and Care Excellence guideline on low back pain and sciatica advises not to offer spinal fusion or disc replacement for people with low back pain.8
The UK guideline on early management of persistent nonspecific low back pain recommends that referral for surgery be reserved for people who do not respond to interdisciplinary rehabilitation.13 A study reported that there are insufficient long-term data to judge the benefits and harms of artificial disc replacement, and it did not recommend the treatment.14
When to consider involving a specialist pain service?
Referral of the patient to a specialist pain service at any stage, including at the initial presentation, should be considered if:
- there is severe pain
- the pain significantly limits his or her lifestyle or daily activities (including sleep disturbance)
- conservative therapies are failing to provide the desired outcome.
Some pain specialist services may provide diagnostic or therapeutic interventional pain management techniques such as lumbar medial branch blocks or sacroiliac joint injection.15 Advanced interventional pain techniques could be considered in some situations. These therapies might include minimally invasive procedures such as pulsed radiofrequency of the dorsal root ganglion or spinal cord stimulation (a neuromodulation technique).16,17 Neuromodulation therapy should be performed by pain specialist physicians suitably trained to deliver this therapy.17
It should be noted that advanced interventional pain techniques are best applied in the context of a biopsychosocial clinic environment, with these therapies supporting physical and cognitive reconditioning alongside optimal use of medications. The evidence base is still under review for these advanced therapies, and they need to be rationally used and individualised to each patient.
Conclusion
Sciatica is common and usually self-limiting; however, in some circumstances it can lead to significant comorbidity and suffering. It is for this reason that all medical practitioners managing people with sciatica should be comfortable with assessing and treating the condition, as well as describing it using the appropriate terminology. PMT
References