A 38-year-old woman with chronic low back pain

Dr Menon is a Specialist Anaesthetist and Pain Medicine Physician at Joondalup Health Campus and Sir Charles Gairdner Hospital, Perth. Dr O’Regan is an Addiction Medicine Specialist with Next Step Drug and Alcohol Services, Perth, WA.
Pain
A pain physician and an addiction medicine specialist discuss the management of a 38-year-old woman with a 10-year history of low back pain who continues to experience significant pain despite taking high-dose opioids, diazepam and pregabalin.
- Establishing a good therapeutic relationship, excluding dangerous pathology early and involving multidisciplinary care early will help to optimise long-term outcomes for patients with chronic pain.
- It is useful to consider whether the patient is primarily experiencing nociceptive pain, neuropathic pain or a mix of both types of pain.
- The GP’s role in safer opioid prescribing can include monitoring for signs of overuse, considering using a treatment agreement, seeking the patient’s prescription history and performing urine drug screens.
Picture credit: © F1online/Axel Leschinski/Diomedia.com
Case scenario
Mrs JL, a 38-year-old married woman with a teenaged daughter, presents with a 10-year history of low back pain. The pain dates from a motor vehicle accident in which she was the at-fault driver when taking her daughter to school. After the accident she also developed left leg pain, which was diagnosed as referred pain caused by intervertebral disc protrusion. She was treated with discectomy. Her most recent imaging scans exclude significant pathology.
Mrs JL is taking 175 mg oxycodone daily (comprising modified-release oxycodone hydrochloride 80 mg twice daily and oxycodone hydrochloride 5 mg three times daily for incident pain), diazepam 5 mg three times daily and pregabalin 150 mg twice daily. Despite this, she reports a daily pain score on a visual analogue scale (VAS) of 5 to 8 out of 10.
Mrs JL has a history of epilepsy, diagnosed in her late teens, with the last recorded seizure five years ago. She does not drink alcohol but has smoked on and off since her early 20s. She trained as a nurse but has been unable to return to work since the accident. Her husband, a self-employed plumber, is supportive, attending all doctors’ appointments with her.
How should this patient be managed?
Commentary from a pain physician
By Rajiv Menon
This is a complex case that will require time and care to address and avoid further unhelpful treatments and investigations. Issues to be considered include:
- assessment of patients with low back pain who have no significant imaging findings
- the role (if any) of high-dose opioids in treating a relatively young person with chronic low back pain
- the role of opioid rotation and dose tapering
- pharmacological treatment of mixed nociceptive and neuropathic low back pain
- implementation of a multidisciplinary approach for chronic pain.
The role of the GP is key in managing this patient. Establishing a good therapeutic relationship, excluding dangerous pathology early and involving multidisciplinary care early will help the GP set the tone for long-term improvements for this patient.
Assessing the cause of pain
Ongoing low back pain, with or without radicular-type symptoms but with no imaging findings, is a common presentation to GPs and pain clinics. Imaging findings and clinical features often correlate poorly in patients with chronic low back pain. Clinical assessment can help to look for other causes of the pain, apart from intervertebral disc disease, which include disorders of the facet joints, sacroiliac joint disease, cluneal nerve entrapment and pain arising from spasm and dysfunction of the muscular structures of the lower back. Furthermore, it should be considered that leg pain may arise from leg structures, rather than representing referred pain from the lower back.
In formulating a management plan, it is also useful to consider whether the patient is complaining primarily of nociceptive pain, neuropathic pain or, as is common, a mix of both types of pain. This can be assessed by thorough history taking that includes the character of the pain, exacerbating and relieving factors, association with particular activities, positions and times of day, and response to treatments. Examination should include neurological assessment, including identification of any sensory abnormalities such as allodynia or hyperalgesia.
It is also important at this stage to exclude ‘red flag’ pathology, such as fractures, infection or cancer. Identification of ‘yellow flags’, such as anxiety, depression, secondary gain, poor coping strategies and litigation/compensation should be picked up here if possible, as they may need to be specifically addressed.
Pharmacological management
A patient with a 10-year history of low back pain is likely to have trialled several different analgesics. Taking a good medication history can be useful. The effectiveness of analgesics depends on factors such as dose, duration of treatment, interaction with other agents and the nature of the patient’s pain. In addition, it is not uncommon for chronic pain to change over time. Consequently, previous failed analgesic options may be worth exploring again.
Nonopioid options
Paracetamol and NSAIDs are usually the first-line treatments for many kinds of pain and are likely to have been trialled in this patient previously. Recent evidence indicates that paracetamol does not have a significant effect on chronic low back pain, and it is likely to be of less benefit in this patient. NSAIDs can be effective in nociceptive pain but have poor efficacy in neuropathic pain. Providing the patient has no contraindications, it would be worthwhile trialling a COX-2 inhibitor such as celecoxib, which has slightly fewer gastrointestinal adverse effects compared with nonspecific NSAIDs. If effective, celecoxib could be continued at a low dose, or used in higher doses for exacerbations of pain (up to 200 mg twice daily if tolerated).
If history taking and examination indicate that the patient’s referred left leg pain has a neuropathic component then it would be worth exploring antineuropathic therapy with anticonvulsants, tricyclic antidepressants (off-label use) or serotonin and noradrenaline reuptake inhibitors (SNRIs).1-3 Recently published Western Australian guidelines on the treatment of neuropathic pain are a good starting point on the use of antineuropathic agents.4
The anticonvulsants pregabalin and gabapentin are increasingly prescribed for patients with chronic pain (only approved for the treatment of neuropathic pain). Care should be taken in patients with renal dysfunction, as these medications are likely to accumulate if renal excretion is reduced. Adverse effects include sedation and dizziness. These medications also have some observed opioid-sparing effects in patients with acute pain, which may be useful in cases where reducing opioid doses is an important goal. A trial of a daytime dose of pregabalin 75 mg, increasing to 150 mg if tolerated, is reasonable in patients with chronic pain. A reasonable maximum dose of pregabalin in the setting of chronic pain is 300 mg twice daily. Gabapentin, although not available on the PBS for neuropathic pain, can be relatively cheap to source via a private script, and can be used as an alternative to pregabalin.
Nevertheless, a recent randomised controlled trial cast doubt on the use of pregabalin to treat sciatica, and in Mrs JL it may be worth trialling cessation of pregabalin for a short period. Like all anticonvulsants, pregabalin should be tapered gradually.2
Tricyclic antidepressants (TCAs) such as amitriptyline and nortriptyline have a low number needed to treat (NNT) in patients with neuropathic pain, but are often less well tolerated because of adverse effects, such as dry mouth, constipation, sedation, drowsiness and tachycardia.1,5 Special care is needed in using these agents in elderly patients and in those with a low seizure threshold (or underlying seizure disorder such as Mrs JL) or cardiovascular risk factors. If tolerated, TCAs can be very effective in treating neuropathic pain (NNT, 3.6), but they may be less effective for low back pain (off-label use). Amitriptyline provides more sedation and can be given at night if sleep disturbance is a concern in this patient. A reasonable starting dose is 10 mg at night, increasing up to 50 mg if needed. Time to onset of effect can be slow, and a trial over at least two weeks may be worthwhile if tolerated.
SNRIs such as duloxetine (only indicated for diabetic neuropathic pain) and venlafaxine (off-label use) are less likely to cause sedation than TCAs. Duloxetine, in particular, has been shown to help improve pain and function in patients with chronic low back pain, including those with neuropathic leg pain.3,6 These should be considered if anticonvulsants and TCAs are ineffective or poorly tolerated. Note, venlafaxine is contraindicated in patients with an underlying seizure disorder.
Opioids and chronic noncancer pain
Mrs JL’s case can be considered a case of opioid-nonresponsive pain and a ‘failed’ surgical treatment. The harms of continued high-dose opioids in this case clearly outweigh any benefits.
The role of opioids in the treatment of chronic noncancer pain, particularly in the setting of neuropathic pain, has changed in recent practice.7 Although there is some evidence that opioids can improve pain in the short to intermediate term, there is little evidence that opioids play a significant role in improving function in patients with long-term pain. Studies of opioid use in patients with chronic noncancer pain show a mean decrease in pain intensity of 30%, with 50 to 80% of patients developing at least one opioid-related adverse event.8,9,10
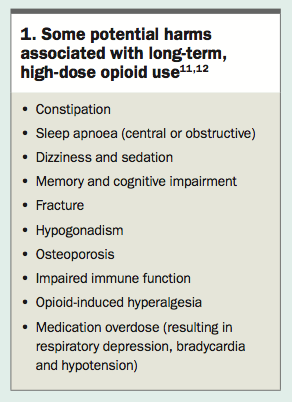
Adverse effects of long-term opioid use include short-term respiratory and gastrointestinal dysfunction and more long-term problems as shown in Box 1.11,12 Opioids are also associated with a significant mortality risk. The risks can increase with longer-term use and high doses. Opioids can also have non-analgesic effects, such as sedation, anxiolysis and euphoria, which can be mistaken for analgesia by patients. Patients who are over-reliant on pharmacotherapy may be ‘chemical copers’, and care should be taken to ensure they are using opioids for the correct reason. They may use opioids to cope with factors such as stress, anxiety and sleep dysfunction. The possibility of addiction also needs to be considered.
{kind=link}
Opioid-dose escalation is a common problem in patients with chronic noncancer pain, and can result from a variety of factors, including decreased efficacy (due to tolerance, opioid-induced hyperalgesia or increasing pain), increased demand due to maladaptive behaviours (such as addiction or diversion) or the effects of dependence and withdrawal. Central and peripheral neuro-adaptation and sensitisation are implicated in most of these factors.
This patient is taking an oral morphine equivalent of 262.5 mg per day, which puts her opioid use well above the high-risk threshold, and it would not be safe for her to continue taking this dose long term.13 A patient taking more than 60 mg of morphine equivalent per day for longer than 60 days requires specialist review. Opioid rotation would be recommended, because incomplete cross tolerance may allow her to obtain better analgesia with a lower dose of another opioid. However, rapid rotation may be difficult to implement given the size of the dose.
Rapid opioid rotation can also be difficult in an outpatient setting. A slow approach with frequent review (e.g. weekly or fortnightly) may be needed to watch for under-dosing (leading to withdrawal) or over-dosing. A recommended dose reduction of the new opioid of 50% (oral morphine equivalent) is appropriate, given incomplete cross tolerance between opioids.8
A possible approach for Mrs JL would be to maximise her nonopioid analgesia (with the strategies outlined above) and to taper her oxycodone slowly. A drop of 10% of her daily dose every fortnight would be a reasonable rate of reduction, but would initially require frequent follow up. Once the oxycodone dose falls below 60 mg per day, it would be feasible to try rotating to an alternative agent such as tapentadol, which would have the added benefit of being more effective in neuropathic pain, as it is both a mu-opioid agonist and noradrenaline reuptake inhibitor.
Multidisciplinary team approach
As mentioned above, many patients with chronic noncancer pain and comorbid opioid dependence are focused on medication for their pain management. However, nonpharmacological approaches to chronic noncancer pain are an important part of evidence-based multidiscipinary care.14 Mrs JL would benefit from a multidisciplinary management plan, delivered through either experienced practitioners in the community or a tertiary pain management unit. Key members of the team would include a physiotherapist, clinical psychologist, occupational therapist, nurse and pain specialist.
It is reasonable to expect that Mrs JL has psychosocial stressors that may be barriers to improving function. Early involvement of a clinical psychologist will be important to screen for psychiatric comorbidities
(especially if these warrant psychiatric involvement), explore family dynamics, and consider implementing psychologicaltherapies, such as cognitive behavioural therapy, which are supported by evidence in patients with chronic pain. This will also provide an opportunity to educate the patient about chronic pain and to emphasise nonpharmacological treatments for pain, which might further reduce her reliance on pharmacotherapy.
A physiotherapist will be valuable not only to establish a plan for rehabilitative exercise and address deconditioning and passive coping strategies, but also to provide education about ‘hurt versus harm’ concepts and to change treatment goals from pain relief to improving function. There is evidence supporting exercise for improving pain levels, physical function and mental health in patients with chronic pain. Transcutaneous electrical nerve stimulation could also be considered as a treatment modality at this time.
A multidisciplinary management plan for chronic low back pain is supported by the highest level of evidence for good outcomes.14 A good therapeutic relationship with a primary care doctor and a multidisciplinary team approach to treatment are likely to lead to a positive outcome, but results are likely to take time.
If Mrs JL is appropriately educated to understand and manage her pain with nonpharmacological methods and to focus on goals of movement and activity rather than pain relief then it should be possible to reduce her reliance on opioids and ultimately to improve her quality of life and long-term function.
Commentary from an addiction medicine specialist
By Richard O’Regan
Mrs JL’s medication regimen, comprising a morphine equivalent dose of 240 mg sustained release and 22.5 mg immediate release combined with high-dose diazepam and pregabalin, presents several risks, including respiratory depression. Benzodiazepines and opioids are well known contributors to overdose, particularly when coprescribed. Mrs JL should be advised about the possibility of overdose and her husband should be made aware of appropriate first aid. In the USA, patients taking significant doses of opioid medication are often provided with naloxone to be administered if overdose is suspected in response to the alarmingly high rate of prescription opioid overdose death in that country.
Signs of problematic medication use
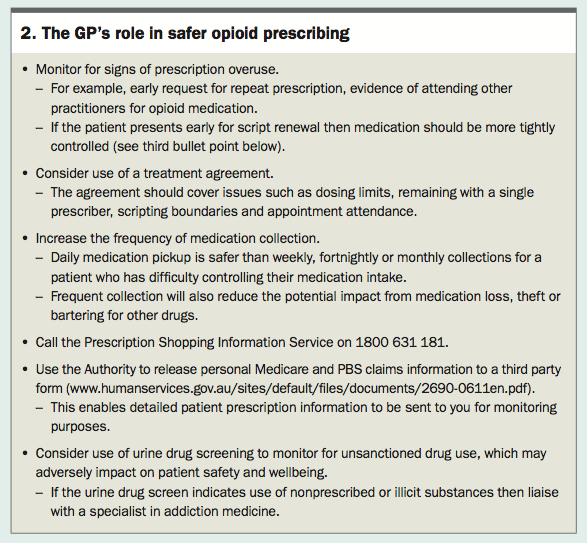
Although Mrs JL does not show behaviours suggesting current or past problematic use of prescription medication, the practitioner should be mindful of the behaviours that signal a problem may be developing. The GP’s role in safer opioid prescribing is summarised in Box 2. It is important to distinguish features of physical dependence (tolerance and withdrawal) from the continuum of aberrant behaviours that result from loss of control in some individuals prescribed long-term opioids. Indicators of concern include:
{kind=link}
- medication access through multiple prescribers, including hospital
- emergency departments
- repeated self-escalation of opioid dose
- running out of medication early
- reports of script loss or theft
- episodes of medication overdose
- recurrent failure to attend specialist appointments.
The risk of problematic medication use is heightened in individuals with a history of substance use, current or past intravenous drug use, prescription forgery, or past treatment with opiate substitution treatment. Mrs JL should also be assessed for anxiety and depression because opioids can be used inappropriately to self-manage negative mood states.
Rotating or ceasing opioids
As Mrs JL continues to have significant pain despite a high dose of oxycodone, an opioid rotation would be an opportunity to reduce the morphine equivalent dose and perhaps open a discussion about a trial of ceasing opioid use completely. This would reduce the risk of harms associated with long-term high-dose opioids (Box 1) while potentially improving overall analgesia. A withdrawal syndrome may occur after regular opioid use over as little as four to eight weeks and may include variable degrees of agitation, anxiety, nausea, vomiting, diarrhoea, yawning, rhinorrhoea, abdominal cramps, myalgia, arthralgia and sweating.
Enhancing the patient’s confidence about ceasing opioid use is crucial and may be achieved by discussing and normalising the expected symptoms of withdrawal, and being sensitive to her anxieties about treatment change. These factors will increase the chance of success. The confidence with which the prescriber can lead such discussions can also have a significant positive impact on success. A written schedule for dose reduction helps both the patient and prescriber remain on target over the weeks and months of dose reduction. Clinicians differ on the preferred rate of dose reduction. Advocates for rapid reduction cite increased chance of success and more rapid resolution of adverse effects. Gradual reduction, however, may be more acceptable to the patient, and thus result in less resistance. Slower reductions may also be associated with less intense withdrawal features, which may suit certain individuals.
Persuading patients about the benefits (potential and actual) of opioid rotation or a trial of opioid dose reduction or cessation in the context of chronic pain is challenging. The prescribed opiate (e.g. oxycodone) may become entrenched as the only solution a patient can or will use, and other legitimate and effective management strategies may be seen as inadequate or ineffective. Patients may become ‘passive’ participants in their pain management, expecting that medication alone will control the pain. In addition, it is not uncommon for patients to use opioid medication to cope with other life problems, such as low mood, grief, anxiety, poor sleep, loneliness and even boredom. If these problems are not addressed then they are likely to persist and contribute to obstacles that must ultimately be overcome before the patient can reduce or cease opioid medication and move forward with their life.
Mrs JL has had 10 years of chronic pain and presumably has been taking prescription opioids for most of this time. The recent scan suggesting she has no significant physical pathology creates an opportunity to discuss dose reduction. An opioid rotation onto opiate substitution treatment (methadone or buprenorphine) is unlikely to be recommended given that Mrs JL does not display any problematic behaviours. Nevertheless, although no other overt risk factors have been identified, the patient’s prescriber needs to be continually vigilant for problematic behaviours that contribute towards ever-increasing doses. Typically, these include self-escalation of daily opioid dose and episodes of early return for script renewal and usually develop over many months or years. Early instances of obtaining medication from other prescribers are seldom identified in a timely manner, although this will change with the introduction of real time Schedule 8 medication monitoring, which is estimated to come into effect in most Australian states and territories in the next 12 to 24 months.PMT
Further reading
References
N Engl J Med 2017; 376: 1111-1120.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.