An elderly woman with acute back pain and osteoporosis

Dr Chen is an Advanced Physician Trainee in geriatric medicine at St Vincent’s Hospital, Melbourne. Associate Professor Katz is a Consultant Geriatrician and Pain Specialist, Director of Geriatric Services at St Vincent’s Hospital, Melbourne; and Director of the Pain Clinic for Older People, Melbourne, Vic.
Osteoporosis
The short- and long-term management of an elderly woman with acute low back pain caused by moving furniture is discussed. A person-centred approach that focuses on active self-care, restoring normal function and use of nonpharmacological therapies is most effective.
- In patients with acute back pain, serious pathology needs to be excluded early.
- The management plan for this case is to restore normal function, treat pain using a combination of nonpharmacological and pharmacological therapies and treat osteoporosis.
- A person-centred approach that encourages active self-care and uses nonpharmacological therapies is most effective.
Case scenario
Erika, a 73-year-old widow of German origin, presents in general practice with severe back pain that started while helping her sister move furniture two weeks ago and is gradually getting worse. She can now barely walk and is brought in by a neighbour who drove her to the surgery. She refuses to go straight to hospital, as recommended by the surgery’s receptionist.
Erika’s past history includes osteoporosis and a cochlear implant for deafness incurred after having worked as a secretary in a heavy industry plant for over 30 years. Erika experienced a similar presentation two years ago, and the radiologist reported no crush fracture but chronic degenerative change of L5/S1 with sclerosis of the end plates, degeneration of the lower lumbar facet joints and a 40% loss of L2 vertebral body height centrally.
During the consultation with the GP, Erika has a pain score of nine out of ten using the Visual Analogue Scale, with pain centred in the lower back with no radiation down either leg. She reports that she cannot get comfortable in bed and has taken some oxycodone her sister gave her. Erika does not take any other medications and has a tendency to be generally nonadherent to medications, having stopped alendronate that was prescribed for her osteoporosis.
How should this patient be managed in the short and long term?
Commentary
Back pain is one of the most common presentations to general practice. About one in four people in Australia will have back pain at some stage in their life, more likely in old age. In most cases, back pain is nonspecific and will settle within a few weeks. The task of managing pain in older patients is often more challenging because of the complexities associated with multiple comorbidities, polypharmacy, physiological changes in drug metabolism and increased likelihood of drug interactions.
In this case scenario, the GP will need to assess the pain and exclude serious pathology. The management plan is to restore normal function, treat pain using a combination of nonpharmacological and pharmacological therapies, and treat osteoporosis. The goals are to optimise functional outcomes, minimise side effects of medications, encourage self-care and prevent further episodes.
Assessment of pain
Most acute back pain is nonspecific and musculoskeletal in origin. Fewer than 1% of patients presenting to primary care will have serious pathology. In most cases, a thorough history and physical examination will obviate the need for radiological assessment. The consultation should be comprehensive, taking into account Erika’s background and social situation. Expectations should be established early.
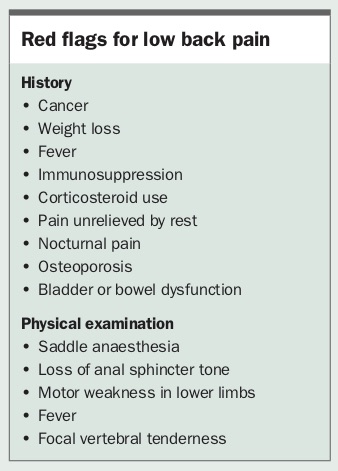
On history taking, Erika reports typical symptoms of a crush fracture with a sudden onset of pain after helping her sister move furniture. She has not been taking alendronate. She reports that the pain is getting worse over the past two weeks and now she can barely walk. This is out of keeping with the natural history of acute back pain. It is important to ascertain what exactly is getting worse. Is it her mood due to pain and lack of sleep? Is there difficulty functioning at home? Any red flags that warrant further evaluation should be elucidated (Box).
{kind=link}
Social factors are important to explore. Although we cannot objectively measure pain, we can assess Erika’s functional ability. If she is unable to manage at home because she cannot perform basic tasks such as getting to the toilet, then she will need hospital admission.
Psychological issues may need to be screened for, as comorbid depression or anxiety is commonly provoked by acute pain and accompanies chronic pain. It is important to interpret the individual’s behaviour in the context of their attitudes towards pain and expectations for treatment. Her stated expectation is that of hospital avoidance, and it may be worthwhile to explore the reasons for her fear of hospitalisation. Erika has a history of nonadherence, and it would be important to address the underlying reasons for this and identify barriers.
Role of imaging
In Erika’s case, the features of concern are her age, the worsening of pain after a fortnight and the presence of nocturnal pain. This may warrant repeat x-rays as an initial step; however, it can be difficult to determine the chronicity of compression fractures on plain radiographs. A comparison with previous imaging or clinical correlation with point tenderness at that region is often relied on. Determining the chronicity of compression fractures can be especially challenging in the elderly and patients with osteoporosis, as bone mineral density appears generally reduced.
Imaging for nonspecific low back pain has not been shown to improve outcomes and carries a greater risk of undergoing invasive procedures.1 Age-related changes are invariably seen, yet their presence may be incidental and unrelated to current pain, and they are not a good predictor of pain severity or progression to chronicity. CT and MRI are not indicated unless there is concern about malignancy or infection, or interventional procedures are being considered.
Acute management
The goal in the first three months is to make the pain tolerable to enable timely return to regular activities. Erika should be counselled about the likely diagnosis and expectation that the pain will ease over the coming weeks, but some pain may persist for some months.
Symptom management comprises both nonpharmacological and pharmacological measures. Erika should be informed that prolonged bed rest is harmful, and she should be encouraged to resume normal activities as tolerated. Conservative approaches, such as hot packs, together with simple analgesics, may facilitate this.
Erika should be safe with her mobility, and a temporary walking aid could be introduced, possibly in collaboration with a physiotherapist. Erika should initiate a gentle mobilisation program, which can be paced over short distances and repeated. She may experience increased pain at times of activity but the goal should be to restore normal function rather than promoting pain avoidance by activity restriction. If disabling pain rendered her immobile, management may need to be escalated to functional rehabilitation in a day centre or as an inpatient.
Pharmacological approach
The traditional approach to pain management has been predominantly pharmacological, based on the WHO analgesic ladder, which is a hierarchical approach to the use of analgesics. Although this has been of benefit in acute pain and cancer pain, its role in the management of back pain and chronic pain is increasingly brought into question. Recent studies question the efficacy of paracetamol as the first step of the ladder in managing back pain and pain of osteoarthritis.2 Second-level agents such as codeine are ineffective in many cases and are becoming less widely available.
There is evidence to support the use of an NSAID in low back pain.1,3 Peptic ulcer, cardiovascular or renal disease and medication interactions are relative contraindications. Commencement of a proton pump inhibitor is advised for gastric mucosal protection together with the NSAID and therapy should be limited to less than two weeks’ duration. Topical NSAIDs may be effective for localised musculoskeletal pain with few systemic side effects.
Opioids constitute the third rung of the ladder but recent evidence does not show superiority over nonopioid analgesics for low back pain.3,4 Moreover, their widespread use has led to an opioid epidemic with addiction problems and rising mortality. Special caution is required with the coadministration of opioid analgesics with benzodiazepines, as the combination is often implicated in prescription drug-related deaths.
A major concern is Erika’s inappropriate use of her sister’s oxycodone on a background of noncompliance to medications prescribed by her doctor. Both Erika and her sister should be advised that sharing medications with others is dangerous, and warned about the harms of taking oxycodone without proper prescription and supervision.
If nonpharmacological and nonopioid analgesics do not give adequate pain relief to enable Erika to resume normal activities, then it may be appropriate to consider a time-limited trial of opioid analgesics, especially if she experienced a favourable response to her sister’s medication. An agreement with Erika should be reached about the short-term use of opioid analgesics. Drawing on her motivation to avoid hospitalisation may allow the clinician to negotiate an early review within a week and limit her supply of oxycodone until such time.
The US Centers for Disease Control and Prevention guidelines recommend that opioid therapy should be initiated with a short-acting agent, rather than a long-acting patch or controlled-release oral preparation.5 The response should be reviewed on a regular basis, and opioid doses exceeding 50mg equivalent of oral morphine per day are not recommended. Generally the duration of therapy would be less than one week. A good rule of thumb is ‘start low, go slow, but go somewhere’. The response should be measured both in terms of pain reduction and function at home. Adverse events of falls and fractures, cognitive impairment, sedation and constipation may outweigh the benefits.
Given the lack of radiation of pain down either leg in this patient, lumbar canal stenosis or sciatica are unlikely. There is no evidence to support the use of neuropathic agents in this case.
Long-term management
Although the prognosis of recovering from an episode of acute back pain is high, recurrent and persistent pain occurs in 20% of patients.6 At the age of 73 years, the average woman in Australia can expect to live another 11 years, thus the priority in Erika’s long-term management is preserving function and preventing the development of recurrent or persistent pain. It should be ensured that she understands the potential benefits of treatment. Erika should be educated on how to manage osteoporosis and prevent falls to reduce her risk of further fractures.
Active self-care is more effective than passive treatment, therefore Erika should be advised to remain active and also be educated about short-term relief options such as use of heat packs and stretching exercises to facilitate physical activity.1,3 Given the severity of Erika’s pain, aquatic therapy may be a gentler form of aerobic exercise compared with land-based exercise in the initial stages. Engagement in group therapies such as self-help groups, pilates or tai chi may reduce the prospects of recurrent back pain and confer additional social aspects contributing to overall wellbeing. Formal cognitive behavioural therapy can be considered if barriers persist or there are ongoing psychosocial issues.3,7
Osteoporosis management
Increased physical activity has cumulative benefits on bone health, falls risk modification and pain reduction. A progressive resistance, weight-bearing and balance exercise program has been shown to halve the fracture risk in people with osteoporosis.8
In addition to physical activity, vitamin D replacement should be considered, aiming for optimal levels of 75 to 100nmol/L to confer protection from both falls and fractures. In community-dwelling adults, dietary intake (three to five serves of calcium-rich food per day) targeting a recommended daily intake of 1200 to 1500mg is preferable because of concerns that supplementation above these levels may be associated with increased risk of coronary artery disease.9
Bisphosphonate therapy is effective in reducing the risk of vertebral fractures by 50 to 70% and also reduces pain.10-12 It is important to explore Erika’s reasons for self-cessation of alendronate. Establish whether this represents a failure to understand the indication of treatment or an issue with tolerability. Common side effects that limit tolerability include dysphagia or oesophagitis.
Erika seems reluctant to take oral therapies. To promote adherence, other options for delivering antiresorptive treatment may be looked at. Erika may favour efficacious and lower frequency treatments such as yearly intravenous zoledronic acid. Denosumab, a RANK-ligand inhibitor, which is given as a six-monthly subcutaneous injection, confers a relative risk reduction of 68% for new vertebral fractures.13
Denosumab and zoledronic acid are subsidised on the PBS for people aged 70 years and older with osteoporosis who have a bone mineral density T-score of -2.5 or less (for denosumab) or -3.0 or less (for zoledronic acid). They are also subsidised for people with established osteoporosis who have fracture due to minimal trauma. The vertebral fracture must have been demonstrated radiologically and is defined as a 20% reduction in vertebral body height. In Erika’s case the 40% loss of vertebral body height would satisfy this criteria.
The role of vertebroplasty in compression fractures is equivocal. Evidence suggests it is no better than placebo and carries the risk of serious adverse events.14,15 It can be considered in the setting of acute compression fractures with incapacitating pain or in people who are unable to tolerate analgesia.
Recurrent and persistent pain in older people
Although counselling for people with acute pain focuses on an expectation that pain will settle over time, this does not apply to chronic pain, which is defined as pain persisting for longer than three months. In this case scenario the expectation is that the pain will persist, which shifts the focus away from minimising pain towards optimising mood, function and quality of life. Optimal management is a balance of effective but tolerable treatment.
Pharmacotherapy has a limited role in persistent pain. There is a paucity of evidence on the use of opioids beyond six months. The average reduction in pain with long-term opioid use is 30%; however, there is no benefit on function, and 80% will experience at least one adverse event.4,16 Long-term use of opioid analgesia can lead to the phenomenon of opioid-induced hyperalgesia, whereby sensitisation within the nervous system from escalating opioid doses results in the paradoxical response of worsening pain. This is distinct from pain associated with opioid tolerance, because in opioid hyperalgesia the pain improves as the opioid dose is reduced.
A multidisciplinary approach that encourages the patient to take an active role in managing their pain is recommended. Enrolment in a community-based, individualised rehabilitation program is validated for improving chronic low back pain.1 A psychologist may provide coping skills, distraction and relaxation techniques to lessen the preoccupation with pain, and teach cognitive restructuring thoughts and beliefs to enhance understanding of the relationship between mood and pain.
As Erika lives alone in her home, home-based supports should be considered. A Webster pack or medication supervision by community nursing services may assist in the safe provision of medications.
Erika may be referred to a chronic pain specialist if, after standard therapies, ongoing symptoms are having a significant impact on her life.
Summary
Back pain is common in older people and the assessment and treatment can be challenging. Current evidence favours nonpharmacological management, self-management and a greater focus on maintenance of function and emotional state over simply eliminating pain. PMT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.