Opioid best practice. New standard: new paradigm
Facilitator and speakers
Associate Professor Ivan L. Rapchuk MD, BSc, FRCPC, FANZCA (Facilitator)
Director of Acute Pain Management Service and Director of Pre-Anaesthetic Clinic at The Prince Charles Hospital, Brisbane; Anaesthetist at Northside Anaesthesia, Brisbane, Qld; Deputy Chair of the Queensland Clinical Network Executive; and Chair of the Opioid Stewardship Working Party.
Dr Monica Steel BaApSci (MedSc), MB BS, MSpMed, FRACGP
GP at Hawthorne Clinic, Balmoral, and the Orthopaedic Fracture Clinic at Mater Adult Hospital, Brisbane, Qld.
Dr Peter Waterhouse MB BS, FANZCA
Anaesthetist at the Queensland Children’s Hospital and in private practice, Brisbane, Qld; and Chair of the Professional Issues Advisory Committee of the Australian Society of Anaesthetists.
Dr Usha Guranathan MB BS, MD, MEpi, FANZCA
Anaesthetist at The Prince Charles Hospital, Brisbane; PhD candidate at the University of Queensland, Brisbane, Qld; and Welfare Officer for the Queensland Regional Committee, Australian and New Zealand College of Anaesthetists.
Dr Dinah Blunt MB ChB, FANZCA, DipClinHypnosis
Anaesthetist and Clinical Hypnotherapist at St Vincent’s Northside Hospital, Brisbane, Qld.
Associate Professor Jennifer Stevens MBChB, FANZCA, FFPMANZCA
Anaesthetist and Pain Medicine Specialist at St Vincent’s Public and Private Hospitals, Sydney; Conjoint Associate Professor at UNSW, Sydney, NSW; and a member of the Australian Commission Working Party on the Australian Commission on Safety and Quality in Health Care Opioid Analgesic Stewardship in Acute Pain Clinical Care Standard.
Dr Tim Tran BPharm, GradCertPharmPrac, MClinPharm, PhD
Senior Clinical Training and Education Pharmacist at Austin Health, Melbourne, Vic.
Ms Ella Raguz BPharm(Hons), MCancerSci
National Clinical Educator for Ramsay Pharmacy; PhD candidate at Monash University, Melbourne, Vic.
Ms Geraldine Griffiths BN, CN, APMS
Clinical Nurse and Coordinator at Wide Bay Hospital and Health Service’s Acute Pain Management Service, Bundaberg, Qld.
This report was written by
Dr Emily Lathlean MB BS, FRACGP Medical Writer/Assistant Editor, MedicineToday
Pain
The Opioid Best Practice – New Standard: New Paradigm educational event was held in Brisbane in March 2022. Hosted by the Opioid Stewardship Working Party (OSWP), the seminar focused on opioid-reduction strategies, safe opioid prescribing, communication between hospitals and GPs, and adapting to the new Opioid Analgesic Stewardship in Acute Pain Clinical Care Standard, which was subsequently published in April 2022. The seminar comprised eight components: the patient journey to surgery, prehabilitation, psychological preparedness for surgery, atypical opioids, hospital to GP communication, a discharge template developed by the OSWP, an introduction to the concepts of the new Clinical Care Standard and two Q&A sessions.
SESSION 1: The patient journey to surgery
The eight weeks before surgery is an important window where GPs can help prepare their patients for surgery and improve postoperative pain management by weaning existing opioid medications and optimising patients’ health generally, according to the first presentation, facilitated by Professor Ivan Rapchuk. However, this can be challenging in general practice and is limited by miscommunication, misconceptions and a lack of time in GP consultations.
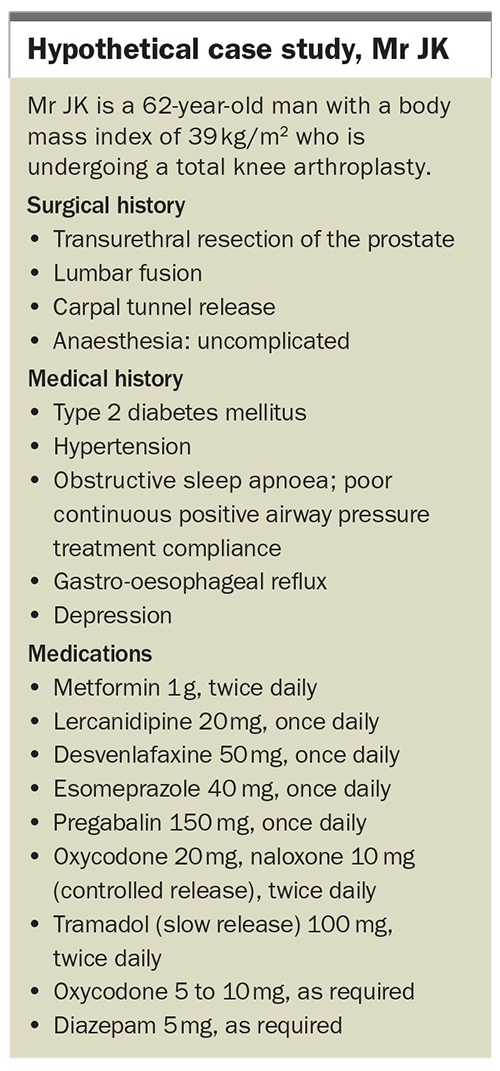
Brisbane-based GP, Dr Monica Steel, and anaesthetist, Dr Peter Waterhouse, discussed a hypothetical case of Mr JK (Case Study Box). Mr JK had chronic knee osteoarthritis with a history of chronic pain, and a history of spinal surgery and comorbidities, including obstructive sleep apnoea and depression.
{kind=link}
Dr Waterhouse noted that Mr JK had several red flags for a complicated postoperative journey, especially for pain management. Ideally, Mr JK should undergo weaning of pain medications eight weeks before surgery, receive preoperative counselling to establish realistic expectations of postoperative pain and optimisation of his comorbidities to reduce his perioperative risks of pain and breathing problems.
Dr Steel acknowledged that although patients with similar complex conditions and medication regimens to Mr JK were common in general practice, their management could be very challenging, and often limited by short consultation times and infrequent appointment attendance.
‘We’re almost constantly looking at "putting out spot fires" because we have 10 or 15 minutes each time,’ Dr Steel said. ‘We’re not able to sit down and give these patients the huge amount of time that we would like to,’ she said, adding that such patients may only be seen once or twice during the preoperative period.
Dr Steel also noted that patients planning to undergo joint replacement surgery often had unrealistic expectations of postsurgical pain outcomes that were difficult to change because their surgeons had given them the impression that their pain would resolve after surgery. Dr Steel said many patients at this point had already given up on nonmedication pain management strategies.
In addition, she said, trying to improve comorbidities and reduce pain medications in this period was difficult as once patients started these medications, it was challenging to convince them to stop taking them. These issues could be exacerbated by mental health difficulties impacting on patients’ motivation and willingness to change their behaviour.
Dr Steel noted also that many GPs didn’t realise the amount of preoperative opioid medications such as that which Mr JK was taking would be an issue and that weaning these would change a patient’s postoperative outcomes. She said education on this would be useful, as would a letter from the surgeon and communication with the anaesthetist preoperatively.
Dr Waterhouse predicted that patients such as Mr JK would be likely to have prolonged admissions due to pain and functional limitations, and be ‘in an even bigger pickle postoperatively than they were preoperatively’ because they were likely to be discharged on even more opioid analgesia than preoperatively to try to manage postoperative pain.
Dr Steel called for more communication from specialists to both patients and GPs regarding patient expectations for postoperative pain, the likely duration of pain postoperatively, the likely duration of the need for opioid analgesia, and guidance about when and how to wean opioid medications.
Dr Waterhouse agreed there currently was significant potential for communication breakdown, especially in the private sector, advocating for the need for additional discharge communication, such as using a nurse- and pharmacist-led team to help execute a postoperative pain management plan after hospital discharge.
SESSION 2: Prehabilitation
The presurgery period is an opportune time to initiate interventions that can reduce perioperative morbidity and help patients withstand postsurgical challenges, according to the second speaker, Dr Usha Gurunathan.
Dr Gurunathan, an anaesthetist at The Prince Charles Hospital, Brisbane, introduced the concept of ‘prehabilitation’: a personalised risk assessment with targeted multimodality intervention aimed to reduce perioperative morbidity. This was an increasingly important concept, she said, especially with the growing prevalence of joint replacement surgeries globally coupled with the rising prevalence of risk factors and comorbidities, e.g. old age, obesity, frailty and polypharmacy. Long waiting periods for joint replacement surgeries, although detrimental to a patient’s health status, had also created an opportune time for its optimisation.
Dr Gurunathan said multimodal interventions were associated with increased compliance compared with single modal interventions, and should incorporate:
- exercise and physical activity: to improve strength, balance, core and respiratory functions
- nutritional optimisation: including increasing anabolism and preventing catabolism, micronutrient optimisation, weight reduction strategies, improving energy reserves and improving protein stores
- optimisation of psychological wellbeing: including stress and anxiety reduction with strategies such as cognitive behavioural therapy and mindfulness.
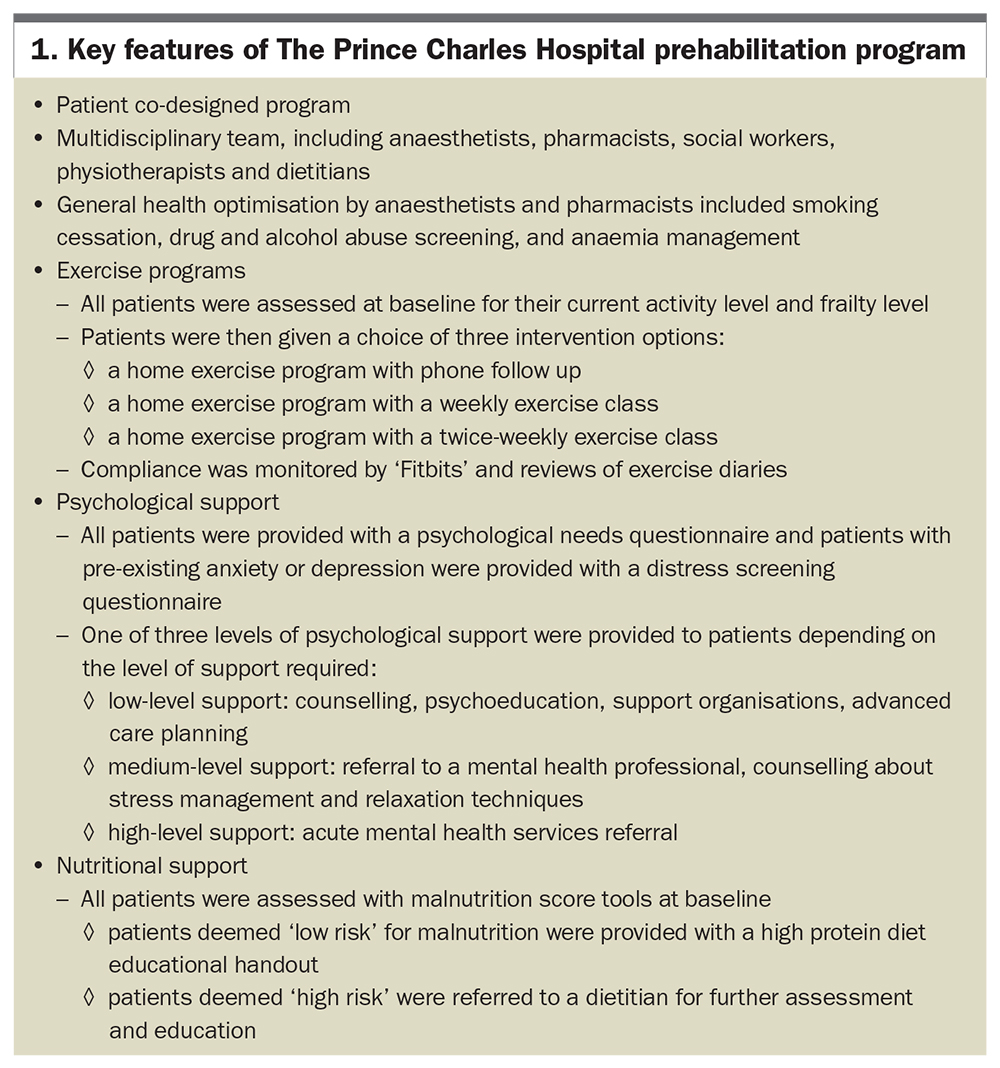
Dr Gurunathan outlined the surgical prehabilitation program at The Prince Charles Hospital and said one of its greatest strengths was that it was a ‘patient co-designed’ program, creating patient empowerment and subsequent compliance. A counselling session at the start of the program enabled the needs and preferences of the patient to be addressed, and the program to be designed based on their capabilities. ‘Ninety percent of the patients rated the program very highly,’ said Dr Gurunathan.
Box 1 lists key features of the program.
{kind=link}
Dr Gurunathan said prehabilitation may have a role in reducing opioid use after surgery, and cited research that found patients who had undergone a prehabilitation program had similar postoperative pain scores to those who hadn’t, but their opioid use was 25% lower.
Individual components of prehabilitation, including exercise, nutrition and weight loss, had also been studied and seemed to be beneficial, Dr Gurunathan said; however, more evidence was needed to confirm variables like optimal duration, intensity and type of exercise, as well as how to design targeted educational programs.
Dr Gurunathan said that preoperative education had been found to reduce length of stay, preoperative anxiety, perioperative pain and readmission rates. However, she noted that preoperative education was often lacking, with some surveys finding fewer than half of patients undergoing arthroplasty received adequate information on pain despite feeling concerned about this and seeking out information; patients who received helpful information had lower pain scores and drug use.
Suggested strategies for preoperative education included:
- discussing prior experiences, preferences and patient expectations
- setting realistic goals about pain management
- discussing analgesic options, including multimodal analgesia
- providing education on risks of opioids and appropriate opioid use
- developing a transitional pain management plan
- tailoring education to age, language and ability to understand
- providing both verbal and printed or video educational materials.
Dr Gurunathan discussed the importance of a close collaboration between primary and secondary models of care in perioperative medicine. She said presurgical optimisation in the primary care setting would enable full utilisation of the preoperative waiting period, patient-centred and place-based care, continuity of care, less reliance on hospital-based care and minimisation of issues relating to geographic location, transport and financial burden.
However, she said there was a ‘guideline to practice gap’ in osteoarthritis management, citing Australian research that found low levels of nonpharmacological treatments used by GPs as first-line management for patients with hip and knee osteoarthritis, compared with higher rates of pharmacological management and surgical referrals.1 Guidelines from the Royal Australian College of General Practitioners (https://www.racgp.org.au/download/Documents/Guidelines/Musculoskeletal/guideline-for-the-management-of-knee-and-hip-oa-2nd-edition.pdf) recommended nonpharmacological strategies as first-line care and strongly recommended against using opioid medications for osteoarthritis, she said.2
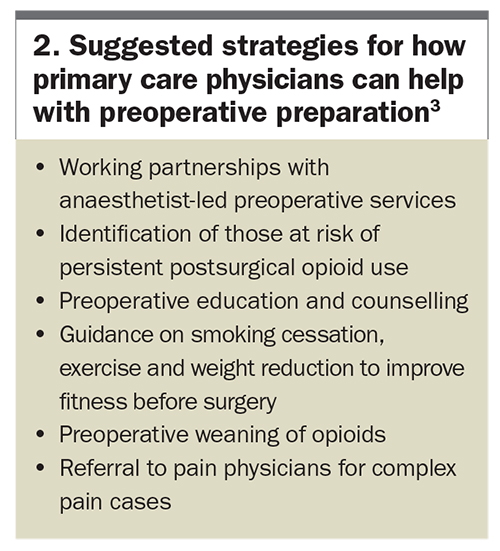
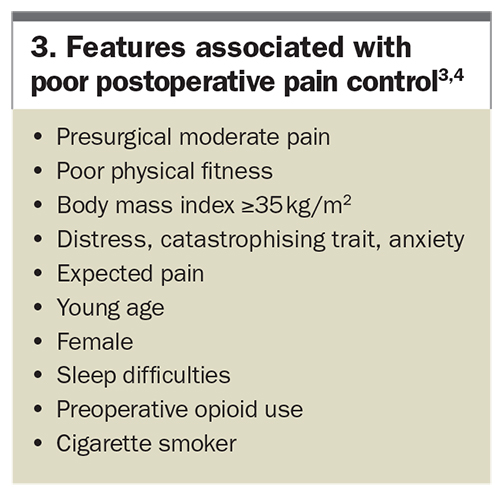
Key strategies suggested by Dr Gurunathan for how primary care physicians could help with preoperative preparation are listed in Box 2. One strategy was the identification of patients at risk of persistent postsurgical opioid use because she said presurgical moderate pain was usually indicative of a neutral or positive pain trajectory. Factors associated with poor postoperative pain control are listed in Box 3.
{kind=link}
{kind=link}
‘If we can identify someone with high pain or moderate pain, perhaps we could implement measures that could change the pain trajectory afterwards,’ Dr Gurunathan said. ‘Pain is not a static concept, it is a dynamic concept.’
SESSION 3: Psychological preparedness for surgery
Patients feeling anxious before surgery can go into a trance-like state, a phenomenon which impairs critical thinking and makes people more open to suggestion, according to Dr Dinah Blunt, an anaesthetist and medical hypnotherapist in Brisbane.
‘It is important to be very careful what you say to these patients because they will take everything literally, they are not going to filter anything,’ Dr Blunt said. ‘Some of the things we say are very well-meaning but the language that we are using actually can have unintended effects on these patients.’
Dr Blunt explained that a hypnotic trance itself was normal and quite common, e.g. it might happen to us when we were watching a movie or on a long car drive, and that during these times we allowed our critical thinking to go ‘offline’.
Dr Blunt referred to the neuro-linguistic programming model, which explains how information is subjected to a range of filters, allowing the brain to decide what information to keep or disregard so that it retains a manageable amount of information. She explained this is why a patient’s impression of what was going on might be completely different from the practitioner’s, and that it could also be significantly influenced by the patient’s emotional and physical state.
Dr Blunt said that patients who were feeling anxious may have impaired critical thinking and generally benefit from certain communication techniques.
‘The subconscious mind is immensely powerful,’ Dr Blunt explained. ‘It is able to do so many things at the same time, it is thinking in abstract, it’s thinking in dreams, emotions and visions, not in a logical, linear fashion. It is unable to process negatives, and this has profound consequences as far as communicating with someone who is tending to go into a trance.’
‘The primary function of the subconscious mind is survival,’ Dr Blunt said, but that when it comes to surgery, a focus on survival and danger could be very unhelpful. Moving a patient to a more positive outlook required clinicians to communicate to both the conscious and subconscious mind, she said.
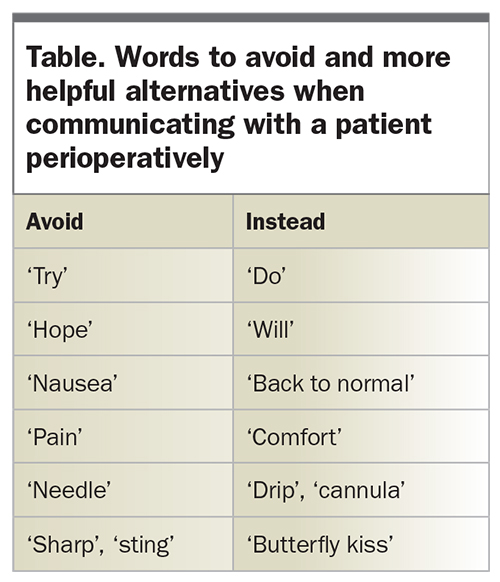
Given the subconscious mind was unable to process negatives, Dr Blunt advised against instructions such as ‘Don’t be scared’. Words to avoid and more helpful alternatives are listed in the Table. Some commonly used phrases during the perioperative period could make erroneous assumptions about patients’ experiences, e.g. asking a patient ‘How nauseous are you?’, when the patient might be feeling malaise but not specifically nausea. She advocated for a focus on comfort and function, and using language that helped patients feel hopeful about their ability to cope with the surgery and recovery.
{kind=link}
The more anxious and distressed the patient or family became, the less they would be able to cope with pain and nausea, follow instructions, undertake rehabilitation, follow their diet, do physiotherapy, etc, Dr Blunt said. She encouraged practitioners to consider that patients might have many worries, not just about postoperative pain or nausea, and advocated for a patient-centred approach to understand their situation and not to make assumptions.
‘A common cause of worry can be a sense of loss of control,’ Dr Blunt said. ‘Providing reframes to the patient can assist with this worry, such as, "Your brain will go to sleep but your body is still directly communicating to the anaesthetist through the monitors; your body is in control." Another strategy was offering patients "binds" – an illusion of choice – e.g. by asking patients whether they would like to sit up or lie down, whether they would like their drip in their left or right arm.’
Dr Blunt emphasised the importance of using the presurgery window to help patients with nutrition, smoking cessation, exercise, optimising medical care and tailoring off opioid medications to improve their postoperative pain relief options.
‘You have a window of opportunity here for patient education, where a patient coming up for surgery has a very strong emotional reason to get themselves to be as healthy as they can,’ Dr Blunt said. ‘You really have to talk to the patients to see what they think are the most important things to look after.’
SESSION 4: Atypical opioids
The concept of multimodal analgesia is that a combination of analgesics with different modes or sites of action can improve analgesia, reduce opioid requirements and reduce adverse effects of opioids in the postoperative period, as explained by Associate Professor Jennifer Stevens, an anaesthetist at St Vincent’s Hospital, Sydney, in her talk on atypical opioids.
Professor Stevens said that this meant the postoperative outcomes we should be focusing on were that a patient’s pain relief was improved and adverse events were fewer.
The concept of ‘mu load’ was discussed, whereby the analgesia and adverse effects of the commonly used intravenous opioids occurred primarily through mu opioid receptors. Atypical opioids, including tramadol, buprenorphine and tapentadol, are opioid medications that are only partial mu-receptor agonists and rely on multiple mechanisms of action.5
‘Buprenorphine in the setting of acute pain is not necessarily an atypical opioid,’ Professor Stevens said. ‘It is a partial potent agonist at the mu opioid receptors, plus active at opioid-receptor-like 1 (ORL-1) receptor… It acts like morphine in acute pain management, but the delivery method (sublingual) is useful compared with intravenous medication. However, there is no benefit respiratory-wise.’
Professor Stevens said tramadol was often not strong enough when compared with tapentadol, a medication that she said had become more popular as drug interactions were much less common. Tapentadol worked at multiple receptors, maintained or improved analgesia, and seemed to do so with lower rates of adverse events, she said. Respiratory depression could occur but much less so than with oxycodone, and its effect on constipation had been found to be similar to that of placebo.6
The choice of immediate- versus slow-release opioid medications was also discussed, with Professor Stevens advocating for immediate-release opioid medications in the setting of acute pain management.
‘I don’t think that there is a huge body of evidence yet about the adverse events of slow-release tapentadol in the acute setting,’ Professor Stevens said. ‘However, the real problem with it is that when you’re giving slow-release in the morning and slow-release at night, there is less to give. By eliminating slow-release [opioid medication], it means I can match the administration of immediate-release [opioid] to what’s happening with the patient and what’s happening with their pain. One of the things that improves patients’ pain relief is a feeling of control.’
Another principle of opioid medication prescribing that Professor Stevens discussed was adequate dosage, noting that younger people required larger doses of opioid medication than older people. The Faculty of Pain Management and Australian and New Zealand College of Anaesthetists Opioid Calculator (available online at http://www.opioidcalculator.com.au) could be used to help with opioid dosing and conversions, she said.
Professor Stevens explained that data from The National Drug and Alcohol Research Council (NDARC), which evaluated supply-adjusted rates of extra-medical pharmaceutical opioid attendances between 2013 and 2018, found tapentadol to be associated with the least attendances of all of the opioids.7 Despite tapentadol sales being the highest of any opioid in Australia in mid-2019, NDARC found very low abuse rates during a survey of intravenous drug users in 2019.8
‘The caveat is… that once it is a "normal" drug, once it’s out there and its supply is even higher, maybe because of its potency and because of its availability we’ll eventually see some abuse,’ Professor Stevens said. ‘But I think we’re getting to a point where we can say maybe that’s actually not going to be the case here, that it hasn’t got particularly likeability for abuse.’
SESSION 5: Hospital to GP communication
Although there have been significant gains over the last couple of years with opioid prescribing, more can be done, according to Dr Tim Tran, pharmacist and Senior Pharmacy Educator at Austin Health, Melbourne, whose talk focused on transitions of care when patients were started on opioid medications in hospital and discharged back to the community.
A 2019 study showed that opioid therapy was initiated in up to 2 million Australian adults each year, Dr Tran said.9 ‘We know that these patients are commonly started on opioids following surgical admissions, and interestingly … the study found that 8% of prescribers were medical interns.’
Dr Tran discussed various interventions that have been studied to try to reduce opioid prescribing, including the implementation of organisational-wide guidelines; statements through peak organisation bodies such as the Australian and New Zealand College of Anaesthetists; education for prescribers, patients, nursing staff and pharmacists; and regulatory changes – e.g. in 2020, the PBS restricted the prescribing of long-acting opioids and reduced pack sizes of these medications.
‘While all of these interventions have been really positive in trying to reduce the flow of opioids, I think from a patient perspective it is really important for us to think about the impact that these changes may have on those patients who do require ongoing supply of opioids and do seek the supply from their GPs,’ Dr Tran said.
Dr Tran outlined a prospective observational study he and fellow researchers undertook at Austin Health, which followed up patients with phone calls three weeks and three months after knee and hip replacement surgery.10 Most patients were supplied with a median of 32 oxycodone pills (1 pill = 5 mg of oxycodone) on discharge. Three weeks' postdischarge, the median remaining number of oxycodone tablets was zero, and most patients (56% of patients overall and 73% of patients who had had total knee replacements) were still taking opioid medications. Nearly half of patients felt that they had received an inadequate supply of opioids from the hospital and around half needed a refill opioid prescription from their GPs. Five percent of opioid-naïve patients developed chronic opioid use.
Dr Tran said the findings highlighted just how much analgesia patients undergoing joint replacement surgery needed on discharge.
‘The take-home messages are that not all patients are oversupplied with opioids following hospital discharge, that it is very difficult to determine the analgesic requirements for some of these patients, and … the need to communicate information to our GPs who are then tasked with the ongoing management of these patients,’ Dr Tran said.
Another study led by Dr Tran evaluated the accuracy of communication from the hospital for 527 patients who were discharged on opioid medications.11 It found 73% of patients were supplied at least one opioid medication on discharge, 73% of whom were opioid naïve. Ten percent of patients did not have a discharge summary. Of those who did, 24% had at least one discrepancy regarding the prescribed opioid medication, such as wrong medication or quantity supplied. Most patients (87%) did not have any opioid management plan documented. Other issues highlighted in feedback from surveyed local GPs included: differing patient expectations regarding how long they would likely require opioid medications, and the difficulty managing patients commenced on opioids, especially for patients who had difficulty weaning off opioid medications and who required additional assistance.
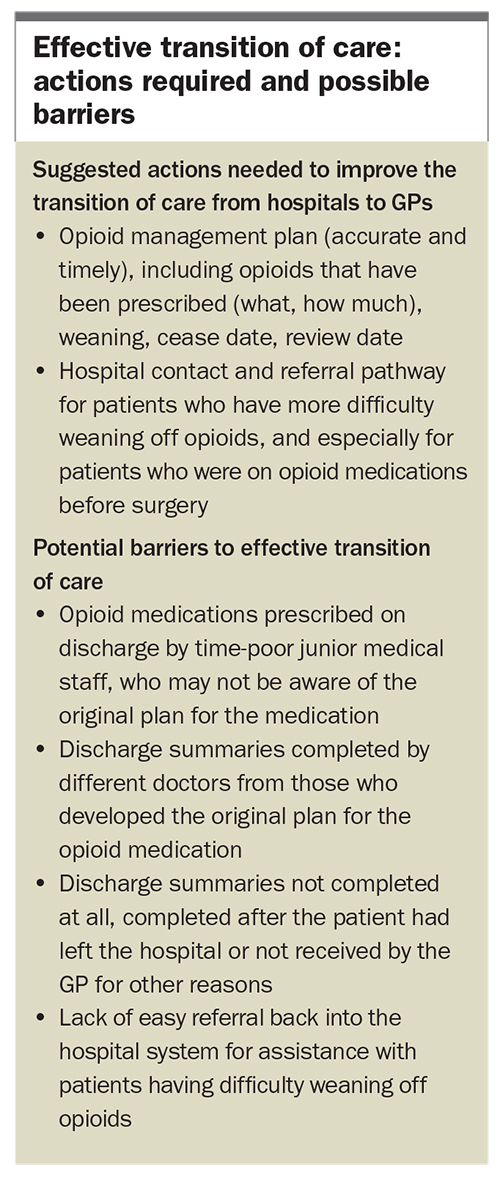
The actions suggested by Dr Tran to improve the transition of care from hospitals to GPs, and possible barriers to effective transition of care are listed in the Box.
{kind=link}
A potential solution, he said, could be a Hospital Outreach Medication Review program, where patients were contacted by a pharmacist soon after discharge to review pain management, and pharmacists would then communicate the pain management plan with the GP, with a transitional care pain clinic also available to review any high-risk postsurgical patients (Figure). Dr Tran shared results from a pilot program trialled at the Austin Hospital of patients following total knee arthroplasty; he acknowledged that while this exact program might not be practical in all settings, the principles could still be helpful to apply. Only around 30% of patients were taking opioid medications three weeks’ postdischarge and needing further supply. Most patients (80%) were satisfied with their supply, despite only 20 pills supplied to patients on discharge. No opioid naïve patients developed chronic opioid use.
{kind=link}
Dr Tran said these findings highlighted the importance of improving the transition of care for postsurgical patients. ‘This can be done through the accurate and timely provision of information on opioids, as well as potentially having an avenue that can support GPs for the more difficult to manage patients,’ he said.
SESSION 6: Discharge template
‘Opioid stewardship can’t be a one size fits all approach, but there are some tools I believe could be implemented and used across all hospital settings to apply some simple opioid stewardship principles,’ said Ms Ella Raguz, a pharmacist and National Clinical Educator with Ramsay Health Care, Melbourne, in her talk.
‘The transfer of patients from hospital back into the community provides a large opportunity for medication errors if communication of a patient’s medications is incomplete or inaccurate,’ Ms Raguz said. ‘Pharmacists play a key role in facilitating discharge and transfer of care to ensure that there is a continuity of optimal medication management for that patient. However,…this is rarely a simple task… and GPs are not receiving the appropriate information to best manage opioid therapy for patients recovering from surgery.’
An opioid tapering plan was only rarely being provided, Ms Raguz explained, and even when it was, patients were only able to digest a limited amount of information at the time of discharge because they were often just focused on going home, she said.
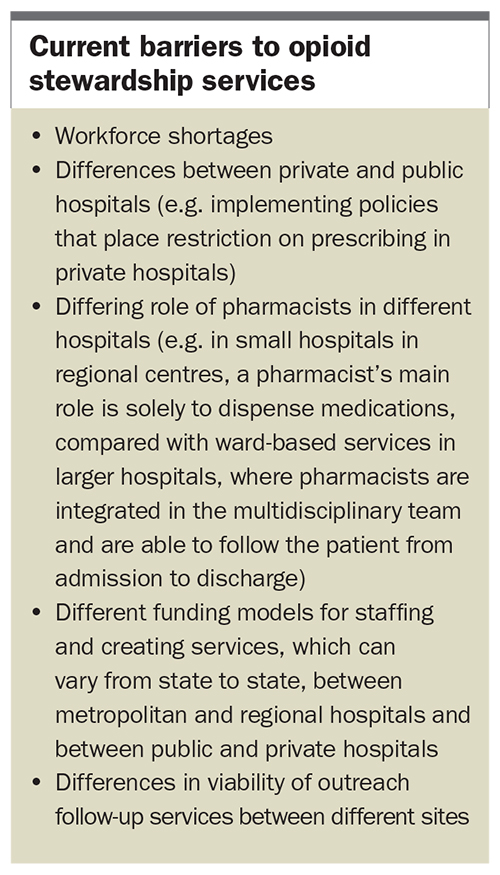
Ms Raguz discussed the concept of an ‘opioid stewardship service’, which had been successfully implemented in some but not all Australian hospitals. In 2018, only 4.5% of Australian hospitals had an opioid stewardship service and these were generally in public hospitals in metropolitan areas. Ms Raguz noted several barriers to opioid stewardship services, as listed in the Barriers to Services Box.
{kind=link}
The OSWP, of which Ms Raguz is a member, has developed a Postoperative Pain Management Plan, which is a template for discharge medications designed to communicate the pain management plan to postsurgery care providers, such as the ward pharmacist, nurse and GP (Figure). It uses a traffic light system to indicate which pain medications should be stopped first, with simple analgesia (paracetamol, anti-inflammatory medications) as ‘green’ options, atypical opioid analgesia (e.g. tramadol and tapentadol) as ‘orange’ medications and typical opioid medications (e.g. oxycodone) as ‘red’ medications. The editable template comes prefilled with information about medication names, strengths, dosage and purpose, with blank spaces for prescribers to write the intended duration of each medication. There is also space for patients to record how many tablets of each opioid medication they are taking daily, explanations about the traffic light system and a list of suggested nonpharmacological pain management strategies.
-Lathlean-OSWP.jpg){kind=link}
‘The patient would get a copy, one would be sent to the GP and a copy would be kept in the patient’s medical record,’ Ms Raguz suggested. ‘Potentially this paperwork could be coded and the data could then be collected if we are looking at the "New Standards" to say that "x" amount of patients got a pain management plan.’
The template could also be easily incorporated in the electronic medical record, or, if the records were paper-based, kept with the patient’s drug chart.
Ms Raguz said the template would provide a central point of information for the patient, pharmacist, nurse, treating doctor and GP, in a way that was low cost, flexible and adaptable, and would facilitate streamlined medication management with minimal added workload.
Ms Raguz said the OSWP hoped this template would become widely used across Australia. A downloadable version of the discharge template is available from the following link: OSWP Post-Operative Pain Management Plan.
Presenting on adoption of the template, Ms Geraldine Griffiths, a clinical nurse with the Acute Pain Management Service at Wide Bay Hospital and Health Service, Bundaberg, said: ‘For me, a few light bulb moments went off when I saw the template – I could see that there were certainly a few gaps in our health service, [which the template would assist addressing].’
‘The template… [provided guidelines] to the prescriber as to what the patient should have on discharge,’ Ms Griffiths said. ‘The traffic light system is great… people are familiar with traffic lights, which is a good safety strategy.’
Ms Griffiths also noted the discharge template’s nonpharmacological strategies, which provided patients with guidance for what to do when they were at home after their procedure, rather than just relying on opioid medications.
‘It’s a good communication tool between the hospital, the patient and the GP as well,’ Ms Griffiths said. ‘I did really want to use this in to our hospital; however, there were a couple of modifications [required] for our hospital.’
Modifications included adapting the Numerical Rating Scale to include a traffic light colour coded Functional Assessment Score, and moving the patient education and patient expectations information to the first page, before any mention of medications, which Ms Griffiths said she hoped would empower patients to use these strategies earlier rather than later.
SESSION 7: New Clinical Standard
The Australian Commission on Safety and Quality in Health Care Opioid Analgesic Stewardship in Acute Pain Clinical Care Standard was launched in April 2022.
Associate Professor Jennifer Stevens, a member of the Commission Working Party, outlined the concepts of the Clinical Care Standard in her presentation; however, because the standard had not yet been published at the time of the seminar, she did not have permission to present its exact wording.
Professor Stevens said the Working Party had ‘very multidisciplinary input’ into these clinical care standards, including surgeons, pharmacists and consumers, and had representation from across Australia. She said the Commission’s role was to develop national safety and quality standards; develop clinical care standards to improve the implementation of evidence-based healthcare; co-ordinate work in specific areas to improve outcomes for patients; and provide information, publications and resources about safety and quality.
Professor Stevens said the Commission would ask practitioners to adopt and document certain standards of care regarding opioid prescribing to meet accreditation standards.
The priorities for the Commission were:
- transfer of care points
- education and training of junior doctors
- development of a Clinical Care Standard
- development of indicators (measures of quality improvement)
- practical assistance for patients, clinicians and health services to help with good decision making.
‘Functional assessment’ was one important concept of the Clinical Care Standard – using a focus on patients’ function and mobility rather than just their pain. Professor Stevens discussed St Vincent’s Hospital’s program, ‘Feeling Hip Again’, as an example of this, involving functional pain assessment, ranging from no limitation to mild or significant limitation due to pain.
Another key concept was avoiding slow-release opioid prescribing, with a push towards strongly encouraging doctors not to prescribe slow-release opioids to opioid-naïve patients, the importance of which she said was clear.
Professor Stevens said that the area in which a patient lives was a factor that contributed to the likelihood of developing chronic opioid use. She gave an example of an audit of the Hunter New England Hospitals that found 22% of patients were still using opioid medications three months after surgery, compared with 3.5% of St Vincent Private Hospital patients (p=0.006).12 This cohort included both opioid-naïve patients and patients who were already taking opioid medications before surgery. Interestingly, there were no differences in pain scores.
Professor Stevens showed data from her hospital showing that slow-release opioid use had reduced both in the hospital and by GPs in the area following education with colleagues, including rehabilitation and geriatric clinicians.
She made reference to the increased difficulties of addressing opioid prescribing problems in private hospitals and quoted data from 2015 to 2016 that found 10% of opioid-naïve patients were still taking opioid medications 90 days or longer postsurgery.13
‘That was one of the things that got me going in this area I guess – the sort of shock that this was happening,’ Professor Stevens said. ‘…We just repeated this [study] and we are now down to zero percent.’
‘It’s possible,’ Professor Stevens said, of reducing chronic opioid use. ‘I think that’s what’s happening around Australia as our prescribing is changing.’
Other data comparing preoperative and postoperative opioid use in regional and inner metropolitan private hospitals highlighted that preoperative opioid use was a major factor in postoperative opioid use, she said.
‘The biggest risk for being on opioids postoperatively is being on opioids preoperatively,’ Professor Stevens said. ‘…[In] most hospitals, two-thirds of those patients will come off [opioids] within three months, but you’re starting way behind, it’s much, much more difficult, and the idea is that we’re not adding to that burden of patients who are on long-term opioids as well.’
Professor Stevens stressed the importance of surgeons also being aware of these strategies. ‘Patients see [surgeons] as being authoritative. They are the ones [who] are operating on the patients, and, as anaesthetists, I think we really need to work on getting our surgeons on board and it’s a real group project, because the surgeons are also communicating with the GPs and I think it just makes that whole nexus much easier for everybody.’
Professor Stevens outlined strategies that could assist with transfer of care, such as anaesthetists writing a pain management plan intraoperatively, giving this to patients after surgery, along with contact information for any questions, and instructing them to take this plan to their GP for ongoing care.
Access the new Clinical Care Standard at: https://www.safetyandquality.gov.au/ publications-and-resources/resource-library/opioid-analgesic-stewardship-acute-pain-clinical-care-standard.
Q&A HIGHLIGHTS
Q: ‘If prehabilitation is so good, why are we having such a tough time selling it to hospitals?’
A: ‘The theory behind it is solid, there is a lot of common sense behind it, but we just have to show the results in terms of its financial outcomes and then it will run in hospitals… There are centres in the UK, Canada, and even in Australia… where prehabilitation has been incorporated as part of the preoperative preparation and running well,’ said Dr Gurunathan.
A: ‘We are conducting a randomised controlled trial in NSW, particularly in regional areas, looking at pharmacy-led deprescribing pre-joint replacement. I think pharmacists are so well placed to do this because they can deal with the complexity of the medications and the communication with the GPs… but also [can] provide broader support to patients during this process and recommend, "Have you thought about doing these exercise programs? Maybe talk to your GPs about doing that." A multidisciplinary [service is] fantastic if you can get it, but I think pharmacists have a pivotal role in this and are grossly underutilised,’ said Professor Stevens.
A: ‘This is mainly for GPs and for assisting transitions of care: as a reminder, you can embed a pharmacist in your GP practice [who] can be the detective when patients come postoperatively as well, because there is going to be a lot of detective work there and GPs are time-poor… [This] may be a solution to some of the problems,’ said an audience member.
Q: ‘What do you see and how do you challenge patients’ expectations in the community and in the hospital?’
A: ‘I think the definition between "pain-free" and "comfort" is very important and surgeons can do a lot better in the way that they phrase [explanations about postoperative outcomes] rather than saying that "this will fix everything". Often these patients are complex and they often have back pain and if they have osteoarthritis in one knee, they probably have osteoarthritis in another knee. So, [it’s better to look] at the outcome for that surgery as "hopefully we can make you more comfortable with this knee",’ said Dr Steel.
A: ‘Absolutely, it’s all expectation. A lot of chronic pain is a learned behaviour… The second thing is, [if a patient] says "I’m really worried about pain postoperatively", the thing to say is, "You will be quite surprised at how comfortable you are postoperatively, and you will be able to get back to normal function as soon as possible, that is the aim of what we’re doing. Yes, you will have some discomfort, you’re supposed to, but this is your body telling you that something has happened and that you should be calming down, taking this seriously, allowing your body time to relax and heal, and we will assist you in keeping you as comfortable as possible, so you are able to move forward with your rehabilitation and getting back to the best function that we can get." It’s this idea of also allowing the patient [to have] some kind of control and to realise that they do have a lot that they can contribute themselves towards their own rehabilitation. Often patients… will appreciate that the fewer drugs the better, the clearer their head, the more likely they are to get on with their rehabilitation. Multimodal [strategies] and reinforcing the use of simple analgesics, simple physical methods,… relaxation techniques are all very helpful and allow the patient to have that sense of control and be part of the whole recovery, rather than being just a victim,’ said Dr Blunt.
Q: ‘What are the panellists’ thoughts on real-time prescription monitoring systems?’
A: ‘I think it makes the conversation easier, so I can… say, "I can’t actually prescribe that for you because I can see you’ve had it prescribed within the last couple of weeks and you’ve gone through above and beyond the recommended dosage, so maybe we need to discuss an alternative."…It’s open to discussion then, it’s not just "I don’t want to prescribe that for you",’ said Dr Steel.
A: ‘I’m not an advocate for mandatory use in every situation… [but] it’s good before you ring up patients or visit them in hospital to know what exactly they’ve had, and sometimes I’m quite surprised by just how many narcotics the patient has been prescribed in the weeks before surgery. If nothing else, it gives you a heads up, and you can initiate a conversation by saying "You’ve had about four boxes of this in the last three months, this is going to impact on how we manage you postoperatively",’ said Dr Waterhouse.
Q: ‘What algorithms would you suggest for GPs to assess the psychosocial risk factors associated with chronic opioid use?’
A: ‘…Anxiety or depression [can] manifest as increased pain… You still need to deal with the anxiety, but it’s not an opioid problem… But yes, absolutely, you can [identify patients] at increased risk, and discuss that with them, and be honest that those sorts of things put them at increased risk; make them aware, educate them, but you can also create an environment [where continuation of opioids is not a ‘quick go-to’],’ said Professor Stevens.
Q: ‘The Commission doesn’t really seem to differentiate between atypical opioids and others, was this discussed at the meetings?’
A: ‘There wasn’t much discussion about typical opioids vs atypical opioids…whichever it is, for acute pain, treatment with opioids should be an acute event, so the intention with both is not to have people on them long-term,’ said Professor Stevens.
The full recording of the seminar is available for viewing at: https://vimeo.com/685349189/c03383e027.
References
9. Lalic S, Ilomäki J, Bell JS, Korhonen MJ, Gisev N. Prevalence and incidence of prescription opioid analgesic use in Australia. Br J Clin Pharmacol 2019; 85: 202-215.