Complex regional pain syndrome. An early diagnosis improves outcomes

Dr Woodgate is Specialist Pain Medicine Physician and Rehabilitation Physician at Austin Health and Alfred Health, Melbourne, and also in private practice at Melbourne Pain Group. Dr Dube is a Specialist Pain Medicine Physician and General Physician at Austin Health and Northern Health, Melbourne, and also in private practice at Mind Body Pain Specialists, Melbourne, Vic.
Pain
The underlying causes of complex regional pain syndrome (CRPS) are poorly understood. Treatment should be patient centred and holistic, with a focus on both physical restoration of function and psychological support. A strong suspicion of CRPS-like features should warrant referral of the patient to a specialised pain team.
- Complex regional pain syndrome (CRPS) is poorly understood and is diagnosed clinically with knowledge of the Budapest criteria.
- Early diagnosis and management of patients with CRPS is crucial to successful recovery.
- Therapies aimed at re-establishing physical and social functioning are associated with the best outcomes in people with CRPS.
- Patients with CRPS-like features should be referred early to a specialised pain service.
Complex regional pain syndrome (CRPS) is a condition that was first described by American physician Silas Weir Mitchell in the 19th Century, after some rather bizarre conditions were observed in veterans of the American Civil War. Historically, it has carried many names, including reflex sympathetic dystrophy, Sudek’s atrophy and causalgia. In 1993, at a consensus conference it was proposed to rename the condition CRPS.1
Today, most cases of CRPS occur after an injury, such as a wrist fracture. Identified triggers can include fractures, sprains and surgery but in rarer cases no trigger is identified. As the name CRPS itself suggests, a region of the body, often an extremity such as a hand, foot or ankle, is affected. Patients often describe persisting pain that is out of keeping with the inciting injury, and associated sensory and motor changes in the affected limb are present.
CRPS is considered a rare condition, affecting between 5 and 26 cases per 100,000 people per year.2 It can occur in people of all ages, but it is rare in the elderly. Women are also more often affected than men. Furthermore, it is more common in upper limb-related trauma.3
‘Beware the strange pain in the strange-looking limb; it’s CRPS until proven otherwise.’ Professor Eric Visser, University of Notre Dame Australia, WA. Australian Pain Society 42nd Annual Scientific Meeting, 2022.
Pathogenesis
CRPS is a pain condition with poorly understood underlying mechanisms and causes. It is not clear why some patients develop such florid signs and symptoms after trauma, which can be very minor. In the past there have been unhelpful attempts to reduce CRPS to a single mechanism, such as reflex sympathetic dystrophy. As the name suggests, the causes are complex; however, it is now generally agreed that multifactorial processes at play, driven by peripheral and central mechanisms (Figure).
{kind=link}
CRPS is likely to start as part of the body’s attempt to heal the initial trauma. The syndrome is heterogenous and several complicated processes likely to be at play in each case; often these underlying causes will change and evolve, even within the same patient over time (hence the wide fluctuation in presentation).4 Processes that have been speculated to be involved include classic inflammation, neurogenic inflammation and changes in the central nervous system that are not helpful.5
Diagnosis
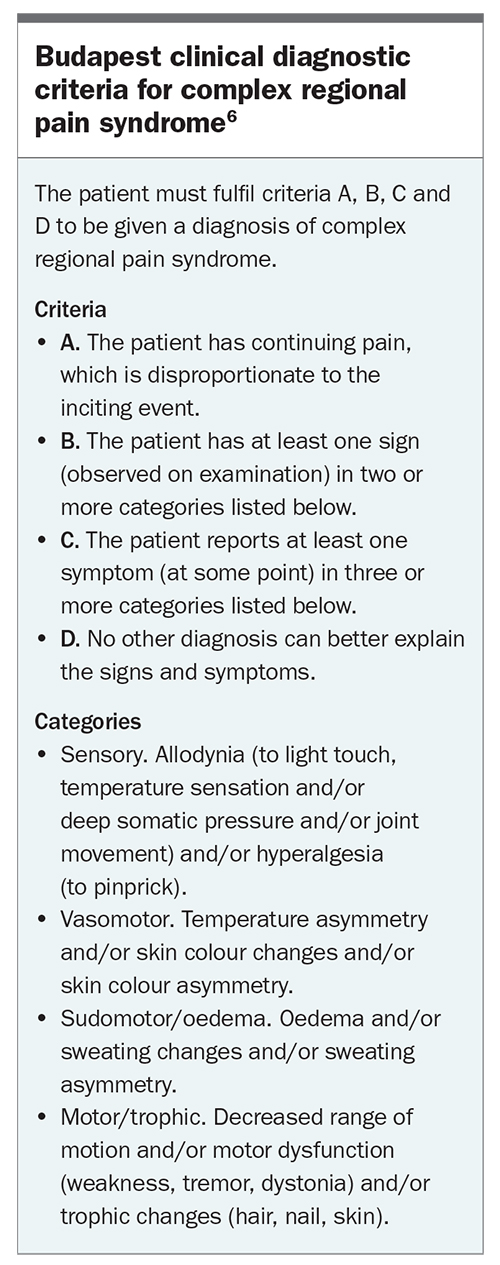
CRPS is a clinical diagnosis that is made after a thorough history and examination of a patient. To make the formal diagnosis of CRPS, the patient needs to fulfil a number of signs and symptoms using the Budapest Criteria (Box).6 CRPS exists on a spectrum and a strong suspicion of CRPS-like features should warrant referral of the patient to a specialised pain team. The most important diagnostic criteria is that the patient should have pain that is out of keeping with the inciting event.7
{kind=link}
Although investigations such as bone scans may suggest the presence of CRPS, they are not enough in themselves to make the diagnosis. Investigations can play an important part in excluding other conditions that may mimic CRPS, such as infection and malunion of fractures.
Treatment
Early diagnosis and management of CRPS is crucial to successful recovery. The strong suspicion of CRPS should trigger urgent attempts to get the patient moving and using the affected limb as much as they are able to. Patients who have acute CRPS respond far more favourably to treatment than those with persistent CRPS, likely due to the entrenchment of changes with the central nervous system and affected limb. This transition to a more prolonged and difficult to treat condition occurs during the first 12 to 18 months after onset, although the exact point at which this demarcation occurs is still being debated.8 As with all complex sociopsychobiomedical conditions, treatment should be patient centred and holistic, with a focus on both physical restoration of function and psychological support during what can be a bewildering and confusing situation for patients.
First-line treatment is early rehabilitation aimed at restoring function to the affected limb.9 Referral of the patient to allied healthcare providers, such as a physical therapist with distal limb expertise to guide physical rehabilitation and a psychologist to provide psychological assessment and support, should be undertaken early. Lack of resolution within a few weeks from initial community management should trigger an urgent referral to the most accessible specialist with pain management expertise. Most pain services will see patients with potential CRPS in an expediated manner.10 Due to the rarity of CRPS, specialised management techniques, both medical and nonmedical, are concentrated within these centres, providing patients with the best chance of recovery. Chronic CRPS is very difficult to treat and, although the largest gains are made early in the syndrome’s course, patients are often left with some residual symptoms.
The pain associated with CRPS can be severe and disabling, limiting progress with rehabilitation. Medications are considered as second-line treatment to assist with restoring function of the affected limb. The choice of agents will depend on the patient’s age, acute or chronic stage of CRPS and the safety profile of the analgesic agent.9 Analgesic prescriptions should focus on functional goals rather than reduction in pain scores and their effectiveness should be regularly monitored. If they are not effective then a patient should be weaned. There is a real paucity of evidence to help give guidance on which medications are most helpful.5 Treatment is therefore largely empirical, with the most commonly used medications being NSAIDs, gabapentinoids, atypical opioids, tricyclic antidepressants and serotonin and noradrenaline reuptake inhibitors.
Vitamin C (500 to 1000 mg orally daily) from the time of injury for 50 days may be considered for the prevention of CRPS.11 It is thought to work by reducing circulating free radicles. Its use has also been extended to early treatment of CRPS; however, there is no evidence for this but it is low risk and patients are nearly always happy to take it.
Smoking is associated with CRPS and is known to impair normal circulation and healing.12 Patients with CRPS who continue to smoke seem to do particularly poorly and encouragement and support to stop smoking is highly recommended.
Use of angiotensin converting enzymes inhibitors increase bradykinin levels, which can worsen neuroinflammation. These medications should be changed to another antihypertensive such as angiotensin receptor blockers.13 Additionally, due to increased sympathetic drive, blood pressure can be significantly elevated in patients with CRPS, which requires treatment.
Other therapies are available at a tertiary healthcare level for the management of CRPS. These include bisphosphonate infusions, ketamine infusions, pain procedures, such as sympathetic nerve blocks, and more advanced invasive therapies such as neuromodulation, which tend to be reserved for patients with CRPS that has not responded adequately to multidisciplinary care.
Outcomes
The outcome of patients who have CRPS is highly variable. Many will have complete recovery without ever receiving a diagnosis of CRPS, whereas others will have ongoing severe life-changing disability. Long-term follow up of patients with CRPS has shown that 30% recovered, 54% remained the same and 16% became worse over a period of five years.14 Almost one-third of patients with CRPS are unable to return back to work. For patients with chronic CRPS the outlook is often quite bleak, with significant entrenched changes within the affected limb, spinal cord and somatosensory cortex.
The risk of recurrence of CRPS ranges between 10 and 30%, and can occur spontaneously or be triggered by surgery or trauma, which can be physical or emotional.15 Patients who have had CRPS previously are at risk of developing CRPS in the same or different limb. These patients should be counselled about the risk of recurrence so that they can inform healthcare providers, as this needs to be taken into account when weighing up the risks and benefits of any proposed invasive procedure to a limb.
Conclusion
CRPS is a pain syndrome with poorly understood underlying causes. It is likely to start as part of the body’s attempt to heal the initial trauma. There can be a wide variance in presentation, even for the same patient. It is diagnosed with knowledge of the Budapest criteria, with a predominant symptom of pain, in combination with other signs and symptoms.
CRPS can be very disabling for patients and they should be supported to urgently reactivate the affected limb within a sociopsychobiomedical framework.
The outcome for patients who have CRPS is highly variable. Early diagnosis and treatment can make a huge difference in the final outcomes for patients with this condition. First-line treatment is early rehabilitation aimed at restoring function to the affected limb. There should be a low threshold for referral of people with CRPS to specialist pain clinics, which will often have expedited pathways for these patients. PMT
COMPETING INTERESTS: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.