Are antipsychotic medications suitable for chronic noncancer pain?

The role of pharmacotherapy in the management of patients with chronic noncancer pain is limited and should be part of an interdisciplinary approach tailored to the individual. There is no rationale or evidence for using antipsychotic drugs in this context.
- Chronic noncancer pain is a complex experience that requires assessment in somatic, psychological and social dimensions, ideally to inform an interdisciplinary approach to management.
- Doctors and patients have relied excessively on medication for treating chronic noncancer pain, despite the moderate track record of commonly used agents – opioids, tricyclic antidepressants, serotonin and noradrenaline reuptake inhibitors and gabapentinoids.
- There is no rationale or evidence for using antipsychotic agents to treat the experience of pain; the increased use of these drugs instead reflects a quest to suppress distressing behaviour.
- The adverse effects of antipsychotic medicines are underappreciated but should temper enthusiasm for their use for any reason other than treating patients with psychotic symptoms.
Picture credit: © Wong Sze Fei/adobe.stock.com Model used for illustrative purposes only.
The antipsychotic class of drugs was developed and registered to treat patients experiencing the symptoms of psychotic disorders, such as hallucinations, delusions and abnormal thought patterns, and for sedation of seriously agitated and disturbed patients. However, the uses of antipsychotic drugs have broadened considerably, especially since the advent of the newer so-called atypical antipsychotics, to include treating patients with anxiety, any degree of agitation or behavioural disturbances, and for sedation more broadly.
Another increasing trend is the use of antipsychotic drugs for patients experiencing chronic noncancer pain (CNCP) – but do these drugs have a useful role in this context? If antipsychotic drugs are being considered for patients with CNCP, it suggests that any treatments offered previously have been ineffective. Before embarking on treatment that appears to be radical and of uncertain rationale, it should be checked whether more conventional elements of a management plan for patients with CNCP have been considered and implemented.
Chronic noncancer pain
CNCP is now evaluated in a psychosocial biomedical framework, which emphasises that social circumstances and psychological issues, as well as somatic or biomedical contributions, must be considered when assessing the patient. Such issues include depression, excessive alcohol use, legal and insurance matters and socioeconomic stress. Treatable underlying conditions causing pain, such as a mechanical origin of neck pain or osteoarthrosis of the knees, are not ignored, but often a mechanism producing the pain cannot be identified let alone directly treated. Furthermore, the presentation of CNCP is commonly ‘comorbid’ with socioeconomic disadvantage (including changed employment status associated with pain), depression and anxiety, as well as a history of childhood abuse and substance misuse.1
The psychosocial biomedical framework also implies that a multidisciplinary approach to assessment and interdisciplinary management of patients with CNCP, wherein psychological, functional and social issues are assessed by relevant team members, is desirable, rather than relying on any one modality of treatment. Nevertheless, in many cases the mainstay of treatment defaults to medication. It follows that polypharmacy becomes the rule rather than the exception, often alarmingly so. The main drug classes used in this context are opioids (e.g. oxycodone, morphine, tramadol), tricyclic antidepressants (TCAs; e.g. amitriptyline, imipramine), serotonin and noradrenaline reuptake inhibitors (SNRIs; e.g. duloxetine, venlafaxine) and gabapentinoids (pregabalin and gabapentin). These drugs have in common mild to moderate efficacy, and also a high prevalence of cognitive (including attentional and motivational) and affective side effects.
Why might antipsychotic drugs be considered for chronic noncancer pain?
Why might an antipsychotic drug even be under consideration for a patient with CNCP? This question takes us back to assessment of the patient in a psychosocial biomedical framework, to determine both the sources of distress and the extent to which therapy has addressed them. Have physical and psychological interventions been recommended and, if so, what has been the patient’s experience? We know that, unfortunately, most people with CNCP do not access a reasonable chronic pain management program, for multiple reasons including limited availability of such services and their associated costs.2
The response of the individual to previously prescribed pharmacotherapy is critical. What medicines have been used? Have they been tolerated? Did the dose need to be increased? What have been the effects, desired and undesired? ‘Desired’ outcomes include increased physical, emotional and social functioning despite persistence of pain, a reduction in distress and minimisation of adverse drug effects. If these outcomes have not been achieved, a differential diagnostic approach to the noneffectiveness of the regimen might be undertaken. This involves asking multiple questions about previous therapies.
First, what has been the intention of the medicines used to date? Opioids, subject to an ongoing trial of effectiveness in the individual patient, tend to target background pain rather than incident pain (‘flares’ of pain). Gabapentinoids are strictly indicated only for true neuropathic pain and, even then, tend to be of modest efficacy.3 The recommended first-line pharmacotherapies for neuropathic pain are TCAs and SNRIs. TCAs are also often used in low doses to enhance sleep, which is helpful but commonly offset by adverse effects such as dry mouth and urinary retention, especially in the elderly. SNRIs are often used to ‘treat’ sadness, coded as ‘pain’, but with only moderate efficacy in relieving pain, in terms of the numbers needed to treat (NNTs). In a recent systematic review and meta-analysis, the reported NNTs to achieve a 50% reduction in neuropathic pain were 6.4 (95% confidence interval [CI], 5.2–8.4) for SNRIs (mainly duloxetine), 7.7 (95% CI, 6.5–9.4) for pregabalin and 7.2 (95% CI, 5.9–9.21) for gabapentin. The NNT was lower for TCAs (3.6; 95% CI, 3.0–4.4).3
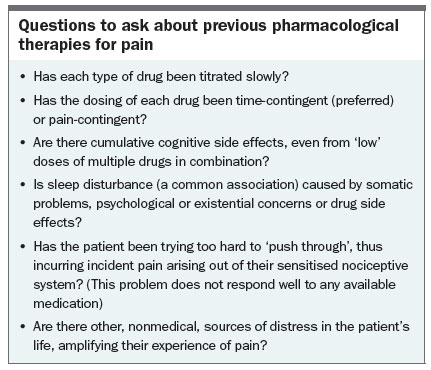
Other questions that should be asked regarding pain therapies are listed in the Box. These are important to answer because improvement is unlikely without a well-constructed approach to the patient and regular review and support. In other words, the reason that antipsychotic medications are being considered for a patient might be the consequence of an insufficient pain management plan resulting from inadequate assessment.
{kind=link}
Evidence for using antipsychotic drugs in chronic noncancer pain
Is there any evidence for using antipsychotic drugs to positively influence the experience of pain in patients with CNCP? The (controversial) answer is both ‘yes’ and ‘no’. A Cochrane review of 770 patients from 11 studies concluded that, although there was some evidence for efficacy of antipsychotics in treating patients with acute or chronic pain, the studies were too heterogeneous to recommend more than ‘more research is needed’.4 A recent review noted that any potential ‘analgesic’ action of first-generation, or typical, antipsychotics, such as chlorpromazine, thioridazine and haloperidol, was limited by adverse effects, including weight gain, hypotension, drowsiness and blurred vision.5 The adverse effects of this class of drugs should lead to reconsideration of adding an antipsychotic medicine to the regimen of a patient with CNCP.
The atypical antipsychotic agents risperidone, olanzapine, quetiapine, ziprasidone and aripiprazole have been used in patients with CNCP, but not in clinical trial circumstances. The atypical antipsychotic group is also associated with adverse reactions, such as weight gain and associated symptoms, drowsiness, heightened risk of falls, cognitive blunting and extrapyramidal manifestations, including exacerbation of Parkinson’s disease symptoms and even tardive dyskinesia. Use of these drugs has been cautioned against, given their uncertain efficacy for treating patients with CNCP and their long-term adverse effects.5
Prescription of antipsychotic drugs
There has been a marked increase in the prescription of antipsychotic drugs. Between 1991 and 2011, the number of antipsychotic prescriptions per 100,000 population rose 2.3-fold in Australia, with prescriptions of atypical antipsychotic drugs, notably olanzapine, quetiapine and risperidone, accounting for most of this increase.6 Much of the increase appears to have been for off-label indications, including sleep disturbances and anxiety, but we suspect that a proportion is for patients with CNCP, despite the lack of evidence of worthwhile effect. Further, the newer atypical antipsychotics (quetiapine, risperidone, olanzapine and aripiprazole) are only PBS-subsidised for various forms of psychosis, including schizophrenia, acute mania and bipolar disorder.
Why has this off-label use of the newer agents occurred? CNCP is prevalent and increasing in Australia; a study in general practice in 2015 found the prevalence to be almost 20%. Osteoarthrosis and back pain were the most common underlying conditions identified.7 Access to services for assistance with managing chronic pain is grossly inadequate.8 Patients often have the expectation that drugs are effective remedies. The failure of opioids as an effective and safe treatment for many patients, now more apparent after a period of liberal use of these drugs, has led to consideration of other classes of psychoactive medicines, such as benzodiazepines and antipsychotics. Many prescribers have considered the atypical antipsychotics to be better tolerated than typical antipsychotics.9 However, as noted, these newer drugs also have a long list of adverse reactions, are possibly more hazardous in overdose6 and are not available via the PBS for CNCP.
Role of antipsychotic drugs in chronic noncancer pain
So, is there a role for antipsychotic drugs in the management of patients experiencing CNCP? There is neither rationale nor evidence for the use of these drugs to treat the symptom of ‘pain’. If a patient with chronic pain should manifest an approved indication for an antipsychotic drug, namely psychosis, there should be no impediment to its use. However, the use of antipsychotics, especially quetiapine, has increased dramatically, well beyond projections for those with psychotic disorders.
A significant proportion of antipsychotic drugs are being prescribed for patients, especially older patients, with unsatisfactory sleep.6 It is well known that poor sleep quality may amplify the experience of pain, but the drugs commonly used in pain management – opioids, TCAs, SNRIs and gabapentinoids – all have drowsiness as a side effect. In the case of aged-care facility residents with sleep disturbances, anxiety and aggressive or disturbing behaviour, it is a common request from the patient, family or staff for ‘something’ to be prescribed. Beyond prolonged-release melatonin, which is well tolerated but not particularly effective as a hypnotic agent, benzodiazepines or sedating antidepressants are unattractive options for their hypnotic properties in the elderly because of the risk of falls, cognitive impairment and, in the case of benzodiazepines, dependence. For an elderly person who complains of pain, but who is also anxious, distressed and difficult to manage, a low dose of an antipsychotic drug may appear to be a more attractive option. However, the reason for such requests is the need for sedation, not pain relief. If the elderly patient also has a degree of delirium, the widespread use of haloperidol or risperidone should be cause for concern, according to a recent randomised, placebo-controlled, dose-adjusted study in the palliative care setting that found a deterioration in patients’ symptoms and distress with use of these agents.10
This again raises the challenging question of how to interpret and assess the complaint of ‘pain’ in an elderly patient with multiple somatic and/or psychiatric comorbidities. Applying a psychosocial biomedical framework can identify a somatic problem that may be treatable either directly or through symptom control with tailored use of established drugs, despite their limitations. However, the framework may also lead to a conclusion that the problem is behavioural. Does that justify the use of an antipsychotic drug? Possibly, but it should be clear – to the prescriber and to the patient, family and carers – that it is brain function, not pain, that is being targeted, and that reduction in symptoms is by no means assured.
Conclusion
CNCP is a complex problem that requires evaluation within a psychosocial biomedical framework. Multidisciplinary assessment and interdisciplinary management may be the ideal, but it is acknowledged that drug therapy may be the only pathway available in many cases. Although the track record of the commonly used drugs – opioids, TCAs, SNRIs and gabapentinoids – is far from impressive, their tailored, judicious use in this context is grounded in rationality and supported by evidence. The same cannot be said of antipsychotics. The increasing use of antipsychotic drugs for patients experiencing pain, especially the elderly, should be seen as a quest for control of distressing behaviour and not as a treatment for pain.PMT
References
- Campbell G, Nielsen S, Bruno R, et al. The Pain and Opioids in Treatment (POINT) study: characteristics of a cohort using opioids to manage chronic non-cancer pain. Pain 2015; 156: 231-242.
- Fashler SR, Cooper LK, Oosenbrug ED, et al. Systematic review of multidisciplinary chronic pain treatment facilities. Pain Res Manag 2016; 2016: 19.
- Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol 2015; 14: 162-173.
- Seidel S, Aigner M, Ossege M, Pernicka E, Wildner B, Sycha T. Antipsychotics for acute and chronic pain in adults. J Pain Symptom Manage 2010; 39: 768-778.
- Khouzam HR. Psychopharmacology of chronic pain: a focus on antidepressants and atypical antipsychotics. Postgrad Med 2016; 128: 323-330.
- Berling I, Buckley NA, Isbister GK. The antipsychotic story: changes in prescriptions and overdose without better safety. Br J Clin Pharmacol 2016; 82: 249-254.
- Henderson JV, Harrison CM, Britt HC, Bayram CF, Miller GC. Prevalence, causes, severity, impact, and management of chronic pain in Australian general practice patients. Pain Med 2013; 14: 1346-1361.
- Hogg MN, Gibson S, Helou A, DeGabriele J, Farrell MJ. Waiting in pain: a systematic investigation into the provision of persistent pain services in Australia. Med J Aust 2012; 196: 386-390.
- Lieberman JA. Atypical antipsychotic drugs as a first-line treatment of schizophrenia: a rationale and hypothesis. J Clin Psychiatry 1996; 57 Suppl 11: 68-71.
- Agar MR, Lawlor PG, Quinn S, et al. Efficacy of oral risperidone, haloperidol, or placebo for symptoms of delirium among patients in palliative care: a randomized clinical trial. JAMA Intern Med 2017; 177: 34-42.
COMPETING INTERESTS: None.