Osteoarthritis: a tailored management approach

Osteoarthritis
Management of patients with osteoarthritis should be tailored to the needs and goals of the individual patient. Key aspects of management are multidisciplinary care, patient education and implementation of referral pathways.
- Pain in osteoarthritis is best understood in the context of a biopsychosocial model.
- The diagnosis of osteoarthritis should be based on a holistic assessment and judicious use of imaging.
- Use of multidisciplinary teams, patient education and lifestyle modification are recommended to promote self-management and improve long-term outcomes.
- Nonpharmacological and pharmacological interventions should be combined with an understanding of the patient’s comorbidities and baseline physical function.
- Surgical intervention should only be considered when conservative management is exhausted.
Osteoarthritis (OA) is a common and disabling condition. The approach to diagnosis and management of OA has changed in recent times with a target of individualised patient care based on patient-specific needs, using a biopsychosocial framework. It is imperative that nonpharmacological interventions are instigated early as the core treatments in the OA armamentarium.
Epidemiology
OA portends a substantial and increasing health burden with significant implications for the individuals affected, healthcare systems and wider socioeconomic costs. OA is a chronic disease that mostly affects the hands, knees and hips. The 2014–15 National Health Survey showed that 2.1 million people in Australia (9% of the population) at all ages have this condition.1 With the population ageing and rates of obesity increasing, the number of people in Australia with OA is expected to increase to almost 3.1 million (12% of the population) by 2030.2 Globally, hip and knee OA were ranked as the 11th highest contributor to global disability and the most notable noncommunicable disease with total disability-adjusted life-years rising by 35% between 1990 and 2015.3,4
OA is placing an increasing burden not only on individuals but also on societies and healthcare systems. Direct healthcare costs for OA were estimated to be over AU$2.1 billion in 2015. Broader economic costs are estimated to be around AU$22 billion annually. Societal costs of OA equate to 0.25% to 0.50% of the gross national product of most western countries.5,6
Pathogenesis
OA is a whole-joint disease, involving structural alterations in the articular cartilage, subchondral bone, ligaments, capsule, synovial membrane and periarticular muscles.7,8 It is an active dynamic alteration arising from an imbalance between repair and breakdown of joint tissues and not a passive degenerative or so-called ‘wear-and-tear’ disease as commonly described.9,10
Pain, joint stiffness and reduced function are the main presenting symptoms of OA.11 Reduced range of motion, crepitus, joint instability (buckling or giving way), swelling, muscle weakness, fatigue and pain-related psychological distress are also often seen in people with OA.12 Pain is the dominant symptom and is a major driver of clinical decision-making and health service use, and is best framed within a biopsychosocial model (Figure).13
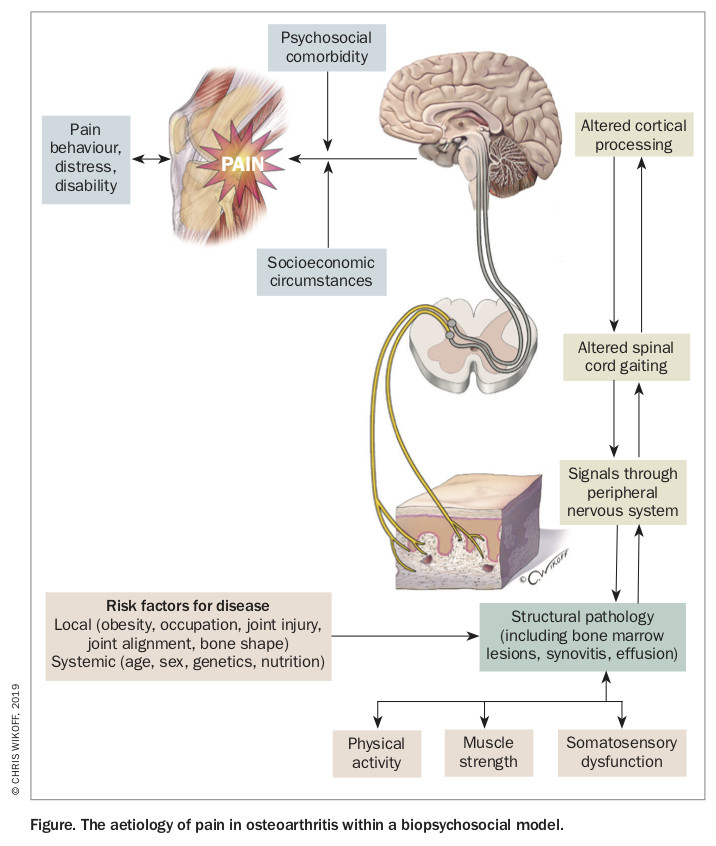{kind=link}
Assessment
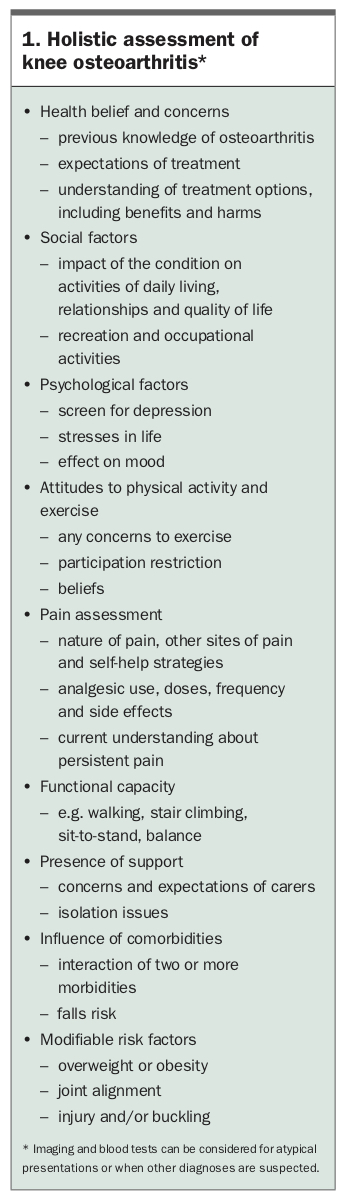
Initial assessment of a patient with OA should include a detailed history and physical examination, including identifying the effect of OA on the person’s function, quality of life, occupation, recreational activities, sleep, mood and relationships (Box 1).14 Whether pain may be referred from surrounding structures, for example, spinal or hip pathology in the setting of knee pain, should also be considered. Further questioning should focus on the impact that comorbidities (e.g. obesity, hypertension, back pain, diabetes, cardiovascular disease, respiratory disease, depression and other mental health conditions, gastrointestinal and renal disease) have on an individual’s overall symptoms and subsequent management course.
{kind=link}
OA is a complex, multifaceted disease in which joint structural damage often does not correlate with the presence or severity of joint pain and disability. A holistic assessment facilitates a collaborative patient-professional partnership in which patients and healthcare professionals make shared decisions related to treatment to improve outcomes.15 Patient preferences for certain types of therapies should be considered, as adherence to treatment recommendations and outcomes can be compromised if the management plan does not meet the patient’s preferences and beliefs.
Patients with knee and/or hip OA should be asked about their knowledge of the disease and treatment alternatives, previous experiences with treatment and expectations of current treatment. The presence of misconceptions, such as ‘exercise will worsen my OA’, or ‘my OA will inevitably get worse’, may hamper the development of an appropriately tailored management plan and limit the success of treatment if not properly identified. Similarly, care should be taken with the use of terminology to describe the nature of findings, such as describing ‘bone on bone’ on imaging or ‘severe OA’, which can potentially trigger unhelpful catastrophic thinking that will influence an individual’s perception of pain and may lead to fear-avoidant behaviour.
The diagnosis of knee or hip OA can be made based on the patient’s symptoms (e.g. persistent knee and/or hip pain, brief morning stiffness and functional limitation) and the results of an adequate physical examination (e.g. crepitus, restricted movement and bony enlargement). Appropriate use of diagnostic criteria, such as those from the American College of Rheumatology or the European League Against Rheumatism for knee osteoarthritis, is recommended (Table).16,17 Plain radiographs are not needed but could be considered for atypical presentations when other diagnoses are suspected or when surgery is indicated.18 Similarly, MRI is not necessary for patients with typical clinical features of OA, unless other pathologies are considered such as avascular necrosis, osteochondritis dissecans or pigmented villonodular synovitis. Degenerative meniscus tears associated with OA are a common feature on such imaging and do not correlate with an individual’s symptoms.
{kind=link}
Management
Care for patients with osteoarthritis should be tailored to the needs and goals of the individual patient. Goals should be specific, measurable, achievable, relevant and have a realistic timeframe (SMART). In the authors’ experience, patients tend to adhere well to treatment plans that are centred around relevant patient goals (e.g. to be able to return to one round of golf pain-free and without the use of a golf cart in six months’ time). Important factors that should be considered by the clinician include the individual’s knowledge of OA and treatment options, current symptoms and functional impairment, mood and sleep disturbance, the presence of comorbidities and their expectations of treatment (and preparedness to engage in treatment).
Management plans should be adaptable and evolve as a patient progresses through treatment. Regular follow-up appointments allow clinicians to monitor and measure progress and encourage ongoing behaviour modification. There should also be consideration of improving patient safety (e.g. falls prevention in a falls-prone individual). Decision-making should be based on the best evidence with prioritisation of patient safety and proactive anticipation of patient needs to be prioritised over a reactive health service.
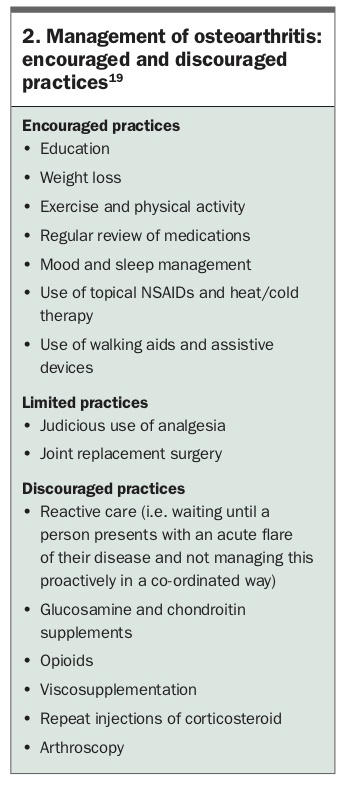
Treatments with the strongest evidence of benefit with minimal risk and cost should be prioritised in the management of OA (Box 2).19 This should be targeted towards the central complaints of pain and functional limitation with management tailored to an individual’s needs. Our healthcare systems should encourage the consistent delivery of interventions that improve consumer knowledge, self-management and healthcare delivery characterised by integrated, multidisciplinary chronic disease management. This model of healthcare delivery is supported by many recent policy changes and will facilitate improved patient outcomes while reducing inappropriate healthcare utilisation and resource waste.20
{kind=link}
Specific management options (including nonpharmacological and pharmacological options) and evidence to support their use are available in the recently released RACGP guidelines.19 Pharmacological treatments can be considered if further pain relief is needed. The RACGP guideline recommends that NSAIDs are taken orally at low doses for short-term use in individual patients, taking into account comorbidities.19 Prescribing doctors should inform patients about, and monitor for, the well-recognised harms of these medications (particularly relating to gastrointestinal and cardiovascular events).
Paracetamol provides minimal short-term benefit for people with osteoarthritis and has an increased risk of adverse events.21 The RACGP guideline does not make a recommendation either for or against the use of paracetamol but rather suggests that it be trialled for a short period, monitored for side effects and discontinued if it is not found to be effective. This advice also stands for topical NSAIDs applied locally to the skin for knee and hand OA.
Corticosteroid injections may be used for short-term pain relief as an adjunct therapy in some people but it is important to recognise that repeated injections should be avoided due to an increased risk of structural disease progression.22 The serotonin and noradrenaline reuptake inhibitor duloxetine can be considered (off-label use) for some patients when other forms of pain relief are inadequate.19
The case presentation in Box 3 illustrates a typical presentation of a patient with osteoarthritis. An approach to the proper management of this case is outlined in the Flowchart.
{kind=link}
Multidisciplinary care
In the authors’ experience, many individuals with OA respond well to treatment using a multidisciplinary team approach. This is because OA is a chronic pain condition associated with comorbidities including psychosocial issues. Although it is recognised that not all patients require such an approach to management, a key role of GPs is to determine whether this is necessary and, if so, to refer the individual to appropriately skilled healthcare professionals in the community or hospital settings. Most people with chronic pain are best managed at the primary care or community level with multidisciplinary support including self-care, but specialist services in hospitals are available to treat more complex patients. The GP is ideally placed to ensure management continuity with a consistent, coherent and collaborative approach to management from all team members that is responsive to the individual’s changing needs. Practice nurses can be invaluable in partnership with the GP in care planning and goal setting.
Useful resources to help facilitate evidence-based multidisciplinary care include the Victorian Model of Care for Osteoarthritis of the hip and knee and the NSW Osteoarthritis Chronic Care program (Box 4). Both of these programs promote, instil and optimise co-ordinated multidisciplinary care and encourage self-management.
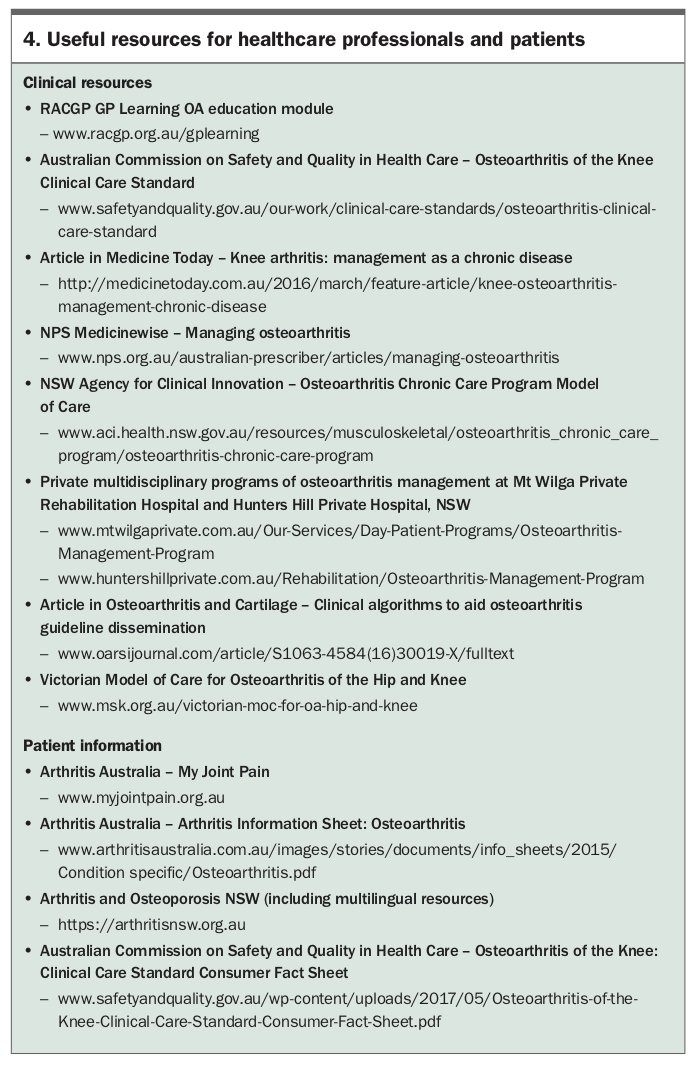{kind=link}
Allied healthcare professionals enhance treatment of OA by adding their expertise to management of the disease. Physiotherapists, exercise physiologists and/or sports and exercise physicians are able to prescribe individualised exercise programs that encourage joint mobility and muscle strengthening. Staying active and increasing muscle strength can help with pain and slow or stop functional decline. Guidelines strongly recommend offering land-based exercise (e.g. walking, muscle strengthening exercise, tai chi) to all people with hip and knee OA.19,23 Exercise should be tailored, considering the individual patient’s preferences, function and comorbidities. Group exercise programs may also be used in the form of tai chi, hydrotherapy and tailored land-based group exercise classes.
Dietitians and/or nutritionists may assist in dietary assessment and management to increase muscle mass (in underweight patients) and weight loss (in overweight patients), as well as management of other comorbidities through better nutrition. Occupational therapists can advise on workplace and home adaptations, activity pacing and energy conservation strategies. Podiatrists and orthotists may be consulted for prescription of appropriately targeted shoe orthotics and braces to improve biomechanics.
Clinical psychology may help with overcoming fear-avoidance behaviours as well as with poor sleep and, if required, treatments for depression to improve a patient’s ability to live with and manage OA. For some patients, referral to a multidisciplinary management program may be warranted particularly if they are having difficulty managing pain despite current best practice.
What not to do
There is a multitude of well-developed osteoarthritis management guidelines available.24 However, some 57% of patients do not receive care concordant with those guidelines.25 Data from Bettering the Evaluation and Care of Health (BEACH) have shown that rates of drug prescription in GP consultations for patients with OA were three times higher than lifestyle management, and more referrals are directed to orthopaedic surgeons (68%) than to physiotherapists (18%).26 The discord between clinical practice and guidelines is thought to be in part due to the trivialisation of OA as a condition of normal ageing, coupled with a perception of limited treatment options.
Efficacious, evidence-based lifestyle behaviour management strategies, such as exercise and weight loss, are underutilised in favour of expensive and reactive treatments.27 Such treatments often have no clinical benefit over placebo, may be harmful and are not cost effective.28 There is robust evidence to suggest that glucosamine, paracetamol, opioids, viscosupplements and arthroscopy, among other popular OA interventions, fall into this category, leading to guidelines recommending against their use in clinical practice.29
Timing and need for referral for surgery
Total joint replacement surgery is a clinically effective and cost-effective treatment for end-stage OA in appropriately selected patients.30,31 It is important to recognise that surgery is not inevitable. The lifetime risk of undergoing total joint replacement is substantially less than the risk of developing symptomatic hip or knee OA. In the UK, the estimated mortality-adjusted lifetime risk of total hip replacement at age 50 years for the year 2005 was 11.6% for women and 7.1% for men.32 For total knee replacement, the risks were 10.8% for women and 8.1% for men.32
GPs should consider referring patients with end-stage OA when all appropriate conservative options, delivered for a reasonable period, have failed. The indication for referral of a patient with osteoarthritis to an orthopaedic surgeon should be based on a substantive decline in quality of life because of established, end-stage joint OA. The hallmarks of end-stage OA include significant joint pain and/or deformity that disrupts normal sleep patterns, which causes a severe reduction in walking distance and a marked restriction of activities of daily living.32 It is important that careful history, examination and investigations (plain radiography) are obtained to reduce the number of patients who undergo inappropriate joint replacement surgery based on minimal symptoms, limited radiographic abnormality and unrealistic expectations (up to 25%).33
Patients with the best outcomes after total joint replacement have significant preoperative radiographic joint change (Kellgren and Lawrence grade 3 or 4), well-controlled comorbidities, a BMI no greater than 30 kg/m2 or no lower than 20 kg/m2 and good mental health status.34-36 Patients planning surgery should maintain the range of motion of their arthritic joint and should engage in as much strengthening and physical activity (e.g. walking, hydrotherapy) as possible.37,38 Not all patients do well even after uncomplicated surgery. At 12 months, after well-performed total joint replacement surgery up to 25% of patients continue to complain of pain and disability.39,40 Careful preoperative patient selection (taking into consideration that poor outcomes are more common in people who have depression, have a history of central sensitisation syndrome with little or no pain, have minimal radiographic disease or are morbidly obese), shared decision-making about surgery and informing patients about realistic outcomes of surgery are required to minimise the likelihood of dissatisfaction. Objective evidence is available that may identify this cohort of patients for whom alternative nonoperative interventions are more appropriate.36
Conclusion
With the ever-increasing rates of OA in our society and the lack of treatment modalities that can halt or reverse the progression of the disease, it is crucial that current management practices are focused towards optimising treatment efficacy through a comprehensive multidisciplinary approach. A biopsychosocial approach to assessment and management should be similar to other chronic pain conditions, in which a tailored, individualised plan is key to success. As symptom control remains a paramount focus in the management of osteoarthritis, the aim is to concentrate on nonpharmacological, noninvasive treatment modalities. PMT
Acknowledgements
Professor Hunter is supported by an NHMRC Practitioner Fellowship. The funding source did not play a role in the development of this article.