Natural compounds for treating pain

The natural compounds found in fruit, vegetables and herbal medicines have emerging scientific evidence of efficacy and safety for treating pain, including neuropathic pain. In the associated field of regenerative medicine concerning amputation pain syndromes, these compounds can potentially enhance tissue regeneration by stem cell expansion and targeted differentiation.
- Natural pain-relieving compounds are found in fruit, vegetables and herbal medicines.
- They exhibit high levels of safety, few side effects and increasing evidence of efficacy.
- The major natural compound classes are polyphenols, polyamines and endocannabinoids.
- Several of these compounds modulate novel pain therapies, such as stem cell treatment, by increasing normal stem cell growth and differentiation and inhibiting cancer stem cells.
Natural compounds constitute an enormous array of substances, from single biomolecules such as vitamins and minerals found in fruit and vegetables, to complex pharmaceutical mixtures of multiple actives found in herbal medicines. They are recognised as historical therapies, often with cultural significance and widespread popular use. Several bioactive principles from herbal medicines have been isolated and purified through chromatographic separation chemistry (e.g. opium poppy), which has led to the development of potent pharmaceutical drugs. The parent source of these compounds is widely used by complementary medicine practitioners, particularly in third world countries. Furthermore, a recent Australian study showed that the overall use of traditional and complementary therapies in Indigenous people with cancer ranges from 19 to 58%.1
Natural compounds and pain management
For acute low-to-moderate pain intensity, treatment often relies on over-the-counter analgesics and NSAIDs to reduce pain. More potent opioid drugs to relieve acute high-intensity inflammatory pain are effective and well accepted by consumers due to the expectation of rapid pain relief. In contrast, pharmaceutical drugs are a first-line choice for managing chronic pain such as neuropathic pain, yet their use may be problematic due to possible significant side effects, potential drug interactions, tolerance and addiction.2 As a consequence, many patients source complementary therapies and ‘try anything to be pain free’, despite a paucity of published scientific evidence.
In western society, consumer use of natural compounds such as vitamin and herbal supplements yields significant revenue. But their popularity often relies on anecdotal evidence, which is largely criticised by medical institutions as lacking adequate high-level evidence. However, increasing evidence from randomised controlled trials is encouraging their use by GPs as adjunct therapies – in addition to first-line pharmaceutical prescription drugs – for the relief and management of pain and other conditions.3 This increase in confidence is driven by improved levels of clinical evidence and underpinned by scientific in vitro studies of ligand-receptor complexes.
Natural compounds and stem cells
The potential therapeutic properties of natural compounds on healthy stem cells, and their corresponding inhibitory effects on cancer stem cells, are being assessed.4 There has been preliminary in vivo evidence demonstrating safety and efficacy using autologous stem cells for treating neuropathic pain.5 Dietary compounds appear to have substantial contributory roles for stem cell behaviour, particularly on stem cell expansion (i.e. increased numbers of cells) and their respective differentiation into the desired tissue type for regenerative medicine. This developing field incorporates molecules and stem cells embedded into bioscaffolds for tissue and organ regeneration.
The goal of regenerative medicine is to repair and replace damaged or lost tissue, and in the case of neuropathic pain, for modulation of pain and restoration of normal neuronal function.
Categories of natural compounds
The natural compounds discussed in this article can be grouped into three categories:
- polyphenols
- polyamines
- endocannabinoids.
Polyphenols
Polyphenol compounds are recognised as a vast source of molecules with antinociceptive and antineuropathic actions.6 There are an estimated 8000 chemical variants of polyphenols from plants. They have a wide margin of safety and are found in fruit, vegetables, grains and herbal condiments, and in professional-grade herbal therapeutic products such as alcohol fluid extracts. Many plant and herbal compounds demonstrate potent multiple properties of anti-inflammatory and anticancer activities, and broad-spectrum antimicrobial actions.7 Due to generations of human exposure through diet and heuristic ‘trial and error’ use, they are generally well tolerated with less or negligible side effects. Several polyphenols have been investigated in vitro for their direct receptor actions and their influence on stem cell lineages.8,9
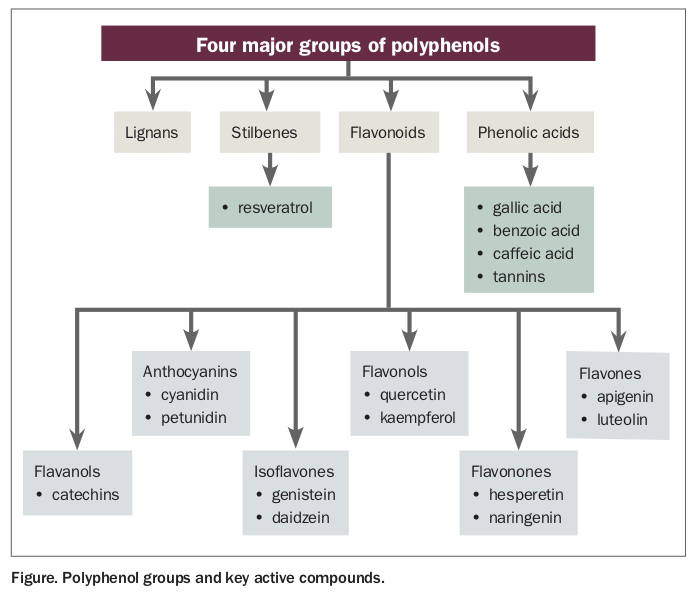
The four major groups of polyphenols are shown in the Figure. Important therapeutic polyphenols include the following:
{kind=link}
- Quercetin-containing foods and herbs are recognised by complementary medicine practitioners as being first-line anti-inflammatory and anticancer food sources. High concentrations of quercetin are found in capers and rocket and (with kaempferol) in raspberry leaf herbal extract. Preliminary safety and efficacy of this herb has been established for the painful precancerous lesions of oral lichen planus using the oral systemic route.10
- Curcumin is derived from turmeric and has anticancer, anti-inflammatory and antineuropathic pain activities.11 Curcumin has multiple molecular effects and inhibits the release of tumour necrosis factor (TNF) alpha and nitric oxide in a dose-dependent manner. Rigorous evaluation in medical oncology trials is ongoing.
- Capsaicin is found in red chilli peppers and capsicums. There is substantial evidence for its use in the treatment of dermal and oral mucosal neuropathic pain states such as postherpetic neuralgia and intraoral trigeminal neuropathy.12 Gingerol (derived from ginger) is a structural analogue of capsaicin and a transient receptor potential vanilloid 1 (TRPV-1) agonist with potential antineuropathic central nervous system effects.13
- Berberine is the active principle of the herb barberry. The isolated compound (20 mg/kg) showed a reduction in cold and mechanical allodynia and was pharmacologically similar to the active control drug amitriptyline (10 mg/kg) in a rat model of neuropathic pain.14
- Genistein is commercially obtained from soybeans. In a rat model of diabetic sciatic nerve injury it relieved allodynia in painful neuropathy by reversing pro-inflammatory cytokines and reactive oxygen species overproduction, and restored the nerve growth factor content in diabetic sciatic nerve.15
- Luteolin is in the flavone class of polyphenols found in celery, thyme, green peppers and chamomile tea. Spinally applied luteolin (0.1 to 1.5 mg) intrathecally or intracerebroventricularly has been shown to attenuate mechanical and cold hyperalgesia in a rat model using a chronic constriction injury (CCI) to the sciatic nerve.16 Spinal action of luteolin is thought to be mediated in part by the GABA-A receptor and opioid receptor. However, results also showed supraspinally applied luteolin had no antihyperalgesic effect on neuropathic pain.16
- Epigallocatechin gallate (EGCG) is found in green tea. An intrathecal injection of EGCG is a Toll-like receptor (TLR-4) inhibitor on neuropathic pain mechanisms (in a rat CCI sciatic nerve model).17 After intrathecal injection of EGCG (1 mg/kg) once daily from one day before to three days after CCI there were decreased expressions of pro-inflammatory cytokines TLR-4, nuclear factor (NF) kappa beta, TNF-alpha and interleukin (IL) 1 beta, and increased anti-inflammatory cytokine IL-10 in the spinal cord with an observed improvement of pain behaviour.17
- Resveratrol is found in berries and red wine and has been shown to attenuate neuropathic pain in a dose-dependent animal model. It has dual pharmacological effects where it prevents expression of pro-inflammatory molecules and promotes expression of anti-inflammatory molecules. Resveratrol promotes expansion and differentiation of osteoblasts from mesenchymal stem cells.8
- Baicalin is an active from the herb skullcap. It has demonstrated an anti-nociceptive effect on histone deacetylase 1 expression in the spinal cord dorsal horn in rats with neuropathic pain.18 Moreover, it promotes neuronal stem cell differentiation.9
Sources of major plant polyphenols and their recommended therapeutic doses are listed in the Table 1.
{kind=link}
Polyamines
Polyamines are a naturally occurring chemical group identified in plant, animal and human species. They are characterised by having two or more NH2 primary amino groups with linear or cyclical structure, which give the compounds a distinctive odour. The compounds are necessary for cellular function and survival. Major compounds are spermine, spermidine, putrescine and cadaverine. Spermine was originally discovered in sperm in the 17th century and is derived chemically from its precursor ornithine and intermediary putrescine (also spermidine). Serum ornithine is found in higher concentrations in patients with persistent musculoskeletal pain.19 Crucial physiological roles include maintenance of cell longevity due to their anti-inflammatory properties, regulating cell metabolism and proliferation.
Polyamine involvement in pain mechanisms includes regulation of calcium, potassium and sodium ion channels and modulating the NMDA receptor. Polyamines are found in broccoli, cauliflower and citrus fruits. A recent study showed a diet that is deficient in polyamines resulted in a rapid reduction of high-intensity acute pain.20 The pharmacology of the polyamines is complex where subcutaneous injections of spermidine or spermine initiate mechanical allodynia and oedema (in a rat model).21 In contrast, co-administration of fentanyl and spermine vastly increases the analgesic efficacy of fentanyl, suggesting potential therapeutic roles of these endogenous substances.22 In addition, spermine induces stem cells to osteogenic differentiation and may have a role in novel cell-based treatments for osteoarthritis.23
Endocannabinoids
The endocannabinoid system occurs in human and mammalian species with important functions in pain, the immune system, appetite and mood. The receptors CB1 and CB2 are expressed in the central nervous system, peripheral nervous system (mainly CB1) and immune system (CB2). Palmitoylethanolamide is an endocannabinoid and chemically, a fatty acid amide. Since its first reported use in 1952 there has been published documentation for its therapeutic utility to treat a wide spectrum of pain states, including neuropathic pain, with a high margin of safety.24,25 The compound is well known as an antineuropathic agent in Europe but is almost unheard of in the US and Australia. It is considered very safe with almost no side effects and has little drug interactions compared with typically used conventional antidepressants and anticonvulsants.26 The safety aspect is highlighted as humans synthesise palmitoylethanolamide endogenously and the chemical is found and processed from natural sources, (i.e. egg yolk, soybean and peanut oil). Its pharmacology is multimodal and targets several receptors including CB1, CB2, PPAR-alpha and TRPV-1. It is one of the few compounds available for pain physicians to reduce noradrenaline release and sympathetically maintained pain.
Other recently identified endogenous lipid molecules include maresins, resolvins and protectins. These bioactive compounds are anti-inflammatory mediators first reported a decade ago.27 They are potent and active at picogram concentrations and have several distinctive chemical isomers named D-series resolvins (resolvin D1 to resolvin D6), protectins (including neuroprotectin D1) and maresins (MaR1 and MaR2). They have both acute and chronic anti-inflammatory actions.28
Discussion
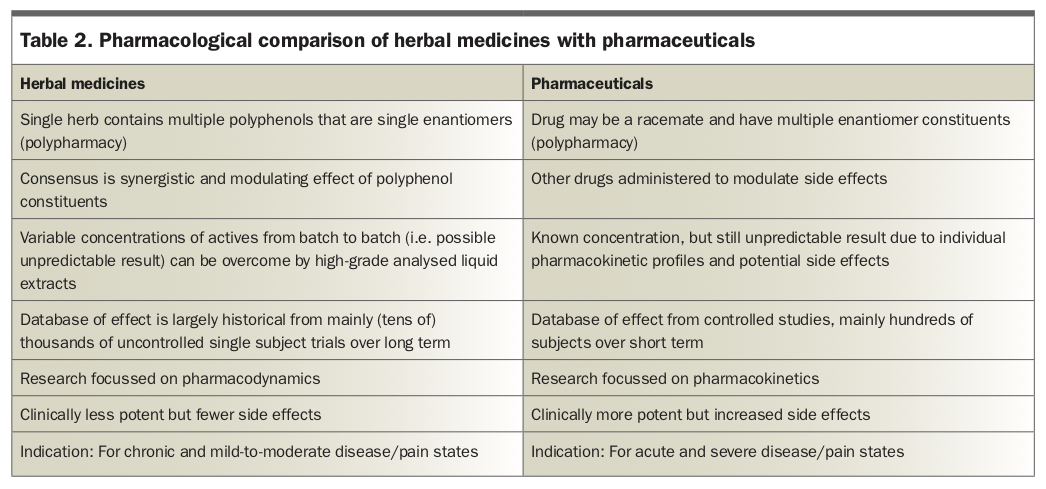
There is increasing evidence for GPs to include natural compounds in the treatment of pain. However, several problems restrict their mainstream clinical use, in particular a lack of level one systematic review evidence. Randomised controlled trials are expensive and pharmaceutical companies that typically sponsor trials cannot patent natural compounds. Another issue is obtaining identical parent herbal formulations in a trial. Herbal extracts have varying levels of bioactives as they may be sourced from different growing regions, soil types and harvesting seasons. These bioactives can be separated and purified by liquid chromatography and molecular identity confirmed by mass spectrometry. However, separation chemistry can be expensive producing high-end-cost single-polyphenol products. Moreover, traditional complementary medicine practitioners argue that multiple active polyphenols in herbs have synergistic action (Table 2).7
{kind=link}
For appropriate clinical use, GPs should have knowledge of therapeutic actions and potential drug interactions, and which compounds have anticoagulant properties in surgery. In Australia, there are high levels of regulatory quality control of herbal supplements by the TGA. Manufacturers of professional-grade herbal products routinely subject the sourced herb and end product to chromatography and mass spectrometry to confirm presence of the polyphenols, determine concentrations of these key actives and identify any problems such as heavy metal contamination or steroid adulteration. Therefore, herbal products manufactured in Australia may be carefully integrated by GPs into chronic pain therapy for improved outcomes. PMT