Chronic noncancer pain: the challenge of implementing opioid guidelines

Dr Hayes is a Specialist Pain Medicine Physician at Hunter Integrated Pain Service, John Hunter Hospita l , N e w c a s tl e , N S W ; a n d D e a n , F a c u l ty o f P a i n Medicine, Australian and New Zealand College of Anaesthetists.
Pain
Guidelines suggest that opioids may be trialled in patients with chronic noncancer pain if expected benefits outweigh the risks. This article addresses how this guidance should be interpreted given the lack of evidence of efficacy and the clear evidence of harm from long-term opioid use.
- An opioid cessation plan should be made whenever opioids are prescribed for patients with acute pain.
- Opioids are no longer considered a core component of treatment of patients with chronic noncancer pain (CNCP). If considering opioid initiation in this setting, discussion with a relevant specialist is recommended.
- A conversation about opioid deprescribing can be initiated with any patient taking opioid maintenance treatment for CNCP.
- Patients can be involved in the deprescribing plan with decisions on whether to undertake a monthly or weekly step down off opioid medications.
- Optimal treatment of CNCP involves supported transition from passively-received treatments such as medications or medical procedures to active self-management.
Picture credit: © Chromorange/Biderbox/Diomedia.com
The Centers for Disease Control and Prevention (CDC) guideline for prescribing opioids for chronic pain was published in March 2016 and seeks to address the highly publicised problems related to the use of prescription opioids in the USA.1 The first of 12 recommendations states: ‘Nonpharmacologic therapy and nonopioid pharmacologic therapy are preferred for chronic pain. Clinicians should consider opioid therapy only if expected benefits for pain and function are anticipated to outweigh risks to the patient.’
There are challenges with translating this recommendation into clinical practice. How strongly should nonpharmacological and nonopioid pharmacological therapy be prioritised? In what circumstances is it reasonable to expect that the benefits of opioid treatment for pain and function might outweigh the risks? This article addresses these questions and provides practical recommendations to support GPs in Australia in treating patients with chronic noncancer pain (CNCP).
Societal context
The magnitude of opioid prescribing and opioid-related harms is considerably greater in the USA than in Australia. Data from 2005 showed that 4 to 5% of the US adult population were prescribed long-term opioids.2 Prescription rates have increased since that time and it was reported in 2008 that the USA, with only 4.6% of the world’s population, used approximately 80% of the global supply of medically prescribed opioids.3 The financial drivers underlying the prescription opioid epidemic are considerable with the global market in 2015 estimated to be worth US$35 billion.4
With such high usage comes significant harm. In 2014, more than 28,000 people died from opioid-related deaths in the USA (87.8 deaths per million persons) and half of those deaths were linked to prescription rather than illicit opioids.5
In Australia, the situation is less extreme with per capita opioid prescribing and opioid-related deaths being approximately one-third of those in the USA. Between 1990 and 2014, opioid dispensing increased almost fourfold in Australia from 4.6 to 17.4 defined daily doses per 1000 inhabitants per day.6 The increase predominantly related to prescription of long-acting opioid formulations for CNCP. In 2013, Australia ranked eighth internationally behind the USA, Canada and five European nations in per capita opioid use; the USA used 51.4 and Australia 17.5 defined daily doses per 1000 inhabitants per day.7 There were 683 opioid-related deaths in Australia in 2011 (30.6 per million persons).8 In the same year, 30% of accidental opioid deaths in people in Australia were due to heroin rather than prescription opioids.8
Opioid recommendations for CNCP in Australia
The Faculty of Pain Medicine (FPM), Australian and New Zealand College of Anaesthetists, has wrestled with the same body of scientific evidence as the CDC and in 2015 produced recommendations on the use of opioid analgesics in patients with CNCP.9 These recommendations state: ‘It is clear that opioid pharmacotherapy cannot be considered to be a core component of the management of CNCP’. In addition ‘The FPM recognises that at the present time opioids are widely prescribed for CNCP despite the lack of clear evidence of efficacy. Given this reality, the following principles are offered to guide their prescription’. These principles include a comprehensive assessment, multimodal therapy and conduct of an opioid trial along with the need to achieve clearly defined goals from the trial before proceeding to maintenance therapy. However, the criteria for commencing an opioid trial are unclear as is the recommended duration of any maintenance therapeutic phase.
A UK perspective
The National Institute for Health and Care Excellence has strong opinions in the discussion of opioids and CNCP. Their November 2016 guidelines address the most common site of CNCP, low back pain.10 These guidelines recommend that opioids are not offered for chronic low back pain. Furthermore, paracetamol alone, antidepressants and anticonvulsants are not recommended for use in patients with low back pain. Judicious use of NSAIDs can be considered. Education, self-management, physical and psychological approaches and return to work are strongly endorsed.
Efficacy and harm
The FPM recommendations affirm that ‘efficacy of opioid therapy is supported by strong evidence from randomised controlled trials in acute pain and from systematic reviews in cancer pain, palliative care and opioid dependency/addiction. In CNCP systematic reviews report modest short term analgesic benefit. However the duration of the randomised controlled trials reviewed (up to four months) was too short to adequately inform the long term role of opioid treatment in CNCP’.9 In fact it is unlikely that the ‘ideal’ randomised controlled trial of sufficient duration will ever be undertaken because of financial and logistic barriers. Population studies show that patients maintained on long-term opioids report high levels of pain and low function.9 Evidence from multidisciplinary group pain programs shows that opioid cessation in that setting can lead to a reduction in pain and improvement in function.9 It has been noted that a focus on pain relief alone via the passive receipt of opioid therapy can distract both patient and prescriber from active self-management strategies.9
The risk of serious harms is dose related. The FPM recommendations endorse a traffic-light approach to categorising risk of harm with a threshold of 40 mg oral morphine equivalent daily dose representing an amber light and moderate risk.9 The threshold of 100 mg oral morphine equivalent daily dose marks the red light zone indicating high risk of harm. Risk is increased in elderly and frail people.
Zones of therapeutic uncertainty
Prescription of opioids for CNCP in the elderly represents a zone of therapeutic uncertainty because of the lack of sufficiently nuanced evidence. Opioid use in this setting is problematic because of the high risk of adverse effects including falls and cognitive impairment. However, there is evidence to support opioid use in palliative care. The uncertainty here relates to the difficulty in defining precisely when a person enters the palliative phase. Before entry to the palliative phase there are differing opinions about the role of opioids but no clear evidence to guide practice. At one end of the spectrum of opinion is the view that it is reasonable to consider opioid maintenance therapy in the elderly only if it is anticipated that the person will die within a 12-month time frame. At the other end of the spectrum is the view that opioid maintenance therapy can be used in an elderly population well before the palliative phase with good effect. Well-designed clinical trials are required to further investigate the multifaceted aspects of opioid use in older persons.
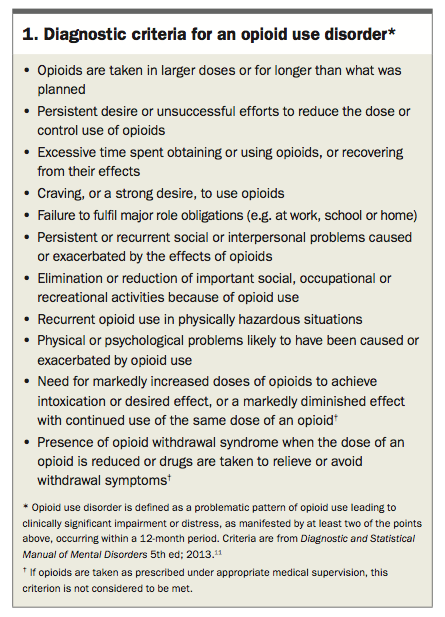
Another zone of uncertainty is the interface between CNCP and opioid use disorder. If the primary problem is CNCP then the usual strategy is to deprescribe opioids. On the other hand if the main issue is opioid use disorder the usual treatment involves opioid maintenance. A practical suggestion here is that when deprescribing opioids in patients with CNCP one should remain vigilant for the emergence of an opioid use disorder as the dominant problem (Box 1).11 If this occurs then switching to an opioid substitution program supervised by an addiction medicine specialist may be warranted.
{kind=link}
A final zone of uncertainty relates to the duration of opioid therapy for patients with complex acute pain. The usual advice for acute pain is to continue opioids for no more than three to seven days. In complex cases, such as multitrauma with interwoven psychosocial factors, duration of opioid treatment is often extended. However, it is worth noting the association between opioid use for more than seven days in workers with acute back injuries and the increased risk of long-term disability.12 Caution is warranted if opioid prescription for acute pain is extended beyond one week.
The language of guideline implementation
Clinician language can be a barrier to or facilitator of the recovery process in people with CNCP. To facilitate the CNCP recovery process, the words of the formulation/diagnosis need to reflect the hope inherent in neuroplasticity and beyond that in biopsychosocial plasticity. Thus ‘pain from severe osteoarthritis of the knee joint’ is not an adequate formulation. Use of such words disempowers the patient and leaves them with little hope of finding strategies to improve the situation. It fails to recognise that another person with the same degree of pathological change on imaging may have no pain. It is better to recognise ‘pain associated with severe osteoarthritis of the knee joint’ and that ‘brain interpretation and nervous system sensitisation’ may be contributing. To ‘retrain the brain and nervous system’ a broad approach is required considering psychological, physical, social and environmental factors. A whole-person approach suitable for people with low literacy has been described with five categories (biomedical, mindbody, connection, activity and nutrition), which can be used to frame assessment and treatment planning.13
If opioids are prescribed in the setting of acute pain, a clearly expressed plan addressing dose and duration of treatment is essential, whether the opioids were initiated in primary care or hospital practice. It needs to be clear that the doctor is in charge of the prescription aspect of the treatment plan and that decisions will be based on a blending of the scientific evidence with the patient’s wishes. Patient agreement is not a necessary prerequisite for opioid deprescribing. A degree of flexibility can be incorporated to enhance patient engagement. ‘Let’s plan to continue the opioid for another week and meet again. At that point it is likely the medication can be stopped, although depending on progress we could consider continuing for a few more days.’
Let us return to the challenge of implementing the recommendation of the CDC guideline that ‘clinicians should consider opioid therapy only if expected benefits for both pain and function are anticipated to outweigh risks’. In reality it is unclear if there are specific, evidence-based, circumstances in which the clinician should rightly expect benefit to outweigh risk. Given this uncertainty, a reasonable interpretation of the CDC guideline is that GPs are advised to discuss strategy with a relevant specialist (pain, addiction medicine or palliative medicine physicians) if considering initiation of opioids for CNCP.
A reduction in opioid initiation does not solve the problem of the so-called ‘lost generation’ who are already taking long-term opioids for CNCP. For this group, opioid deprescribing is generally recommended. It is helpful to recognise previous attempts at weaning and ask about difficulties that arose. The language of television advertising about smoking cessation may be helpful, noting that each attempt is not a failure so much as a valued experience that increases the likelihood of success at the next attempt.
In a tertiary multidisciplinary setting where many patients have been taking relatively high doses of opioids for several years, the usual deprescribing plan involves a monthly step down of 10 to 25% of the starting dose. This achieves cessation in three to nine months. In a primary care setting, a step down each week may be feasible in some situations. A helpful strategy can be to offer the patient the choice of a fast or slow wean. ‘Would you prefer to reduce the dose each month or each week?’ It can also be helpful to mention the possibility of transition to an opioid substitution program supervised by an addiction medicine specialist. ‘Sometimes as the dose is reducing it becomes clear that the main problem is opioid dependency. If that happens then we can ask the local Drug and Alcohol service to advise about a methadone or buprenorphine program.’
Conclusion
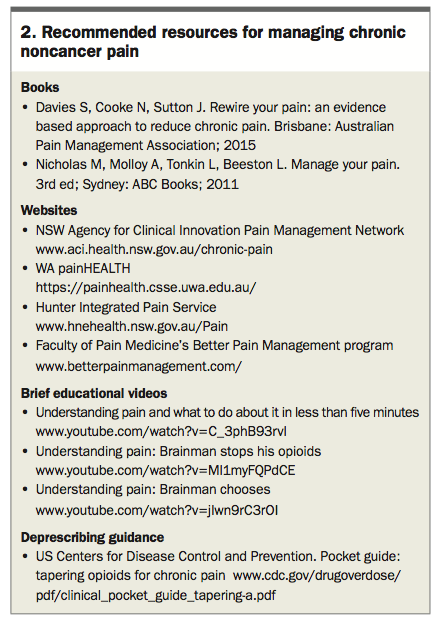
Current opioid guidelines need to be examined with care to distil key messages for use in everyday practice. Nonopioid treatment strategies are more effective and less harmful in people with CNCP. Recommended resources for managing CNCP are listed in Box 2. Evidence suggests that the harms of opioid prescription are likely to outweigh the benefits in these people. Opioid use may lead to less engagement with active self-management of CNCP and poorer outcomes. PMT
{kind=link}
References
London: NICE, 2016. Available online at: www.nice.org.uk/guidance/ng59 (accessed July 2017).
p. 541-560.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.