Shoulder pain: how to assess, when to refer

Dr Brown is an Advanced Trainee in Rheumatology and General Medicine at Southern Adelaide Local Health Network, Flinders Medical Centre, Adelaide. Professor Shanahan is Professor of Musculoskeletal Medicine at Flinders University and Head of Rheumatology at Southern Adelaide Local Health Network, Flinders Medical Centre, Adelaide, SA.
Shoulder injuries and disorders
Pain
Shoulder pain is a common clinical problem in general and specialist practice. Investigation and treatment should be guided by the initial clinical findings and tailored to the patient’s symptoms. Referral for specialist advice is recommended for patients who need surgery or if red flags or refractory symptoms are present.
- Most shoulder problems are identified and managed in the primary care setting.
- Clinical history and examination are integral to making a diagnosis.
- Further investigations can be targeted to patients presenting with red flag features or for evaluation before surgical intervention.
- Specialist referral of the patient should be directed with consideration to the aetiology of the problem and the likely required intervention.
Shoulder pain is a common and often disabling complaint in the Australian community.1 It is the third most common musculoskeletal presentation to primary care and is one of the world’s top 10 contributors to global disability burden.2,3 The diagnosis and management of shoulder pain in general practice is important, as about 14% of patients presenting with shoulder pain will be continuing to receive care at three years, and 22.5% will be referred to a specialist.4 Surveys of GPs reveal uncertainty in the diagnosis and management of shoulder pain leading to a high investigation rate and use of healthcare resources.5
Causes of shoulder pain
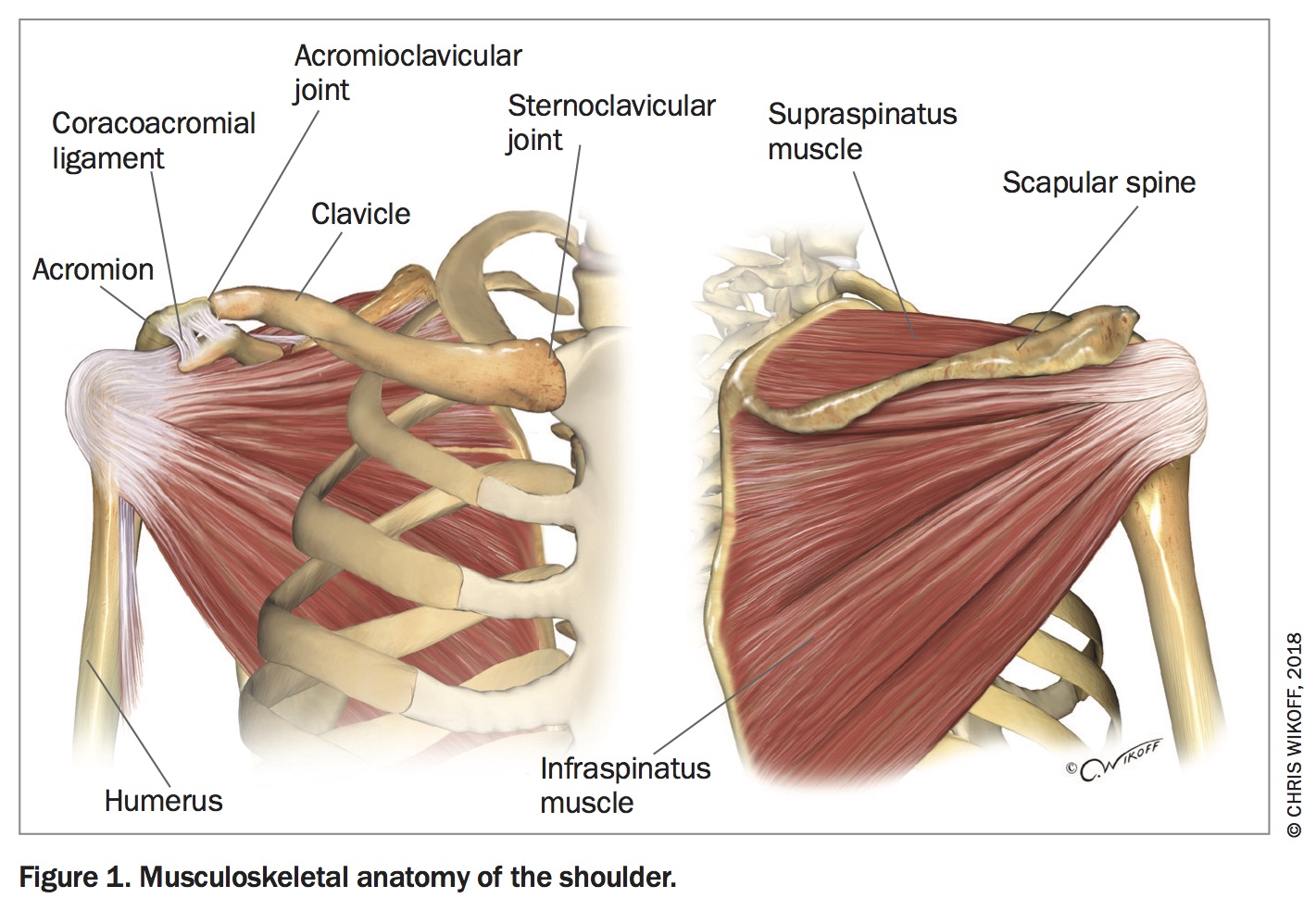
The shoulder is a complex structure designed to provide significant flexibility. The relatively shallow glenohumeral joint is highly dependent on ligaments and tendons for stability, making the shoulder relatively prone to injury and subsequent pain, instability and loss of function. The main components of the shoulder include the glenohumeral joint, which is the primary articulation, the acromioclavicular and sternoclavicular joints, the scapulothoracic articulation, subacromial bursa, synovial capsule and the rotator cuff muscles, which provide dynamic stabilisation of the shoulder joint (Figure 1).
{kind=link}
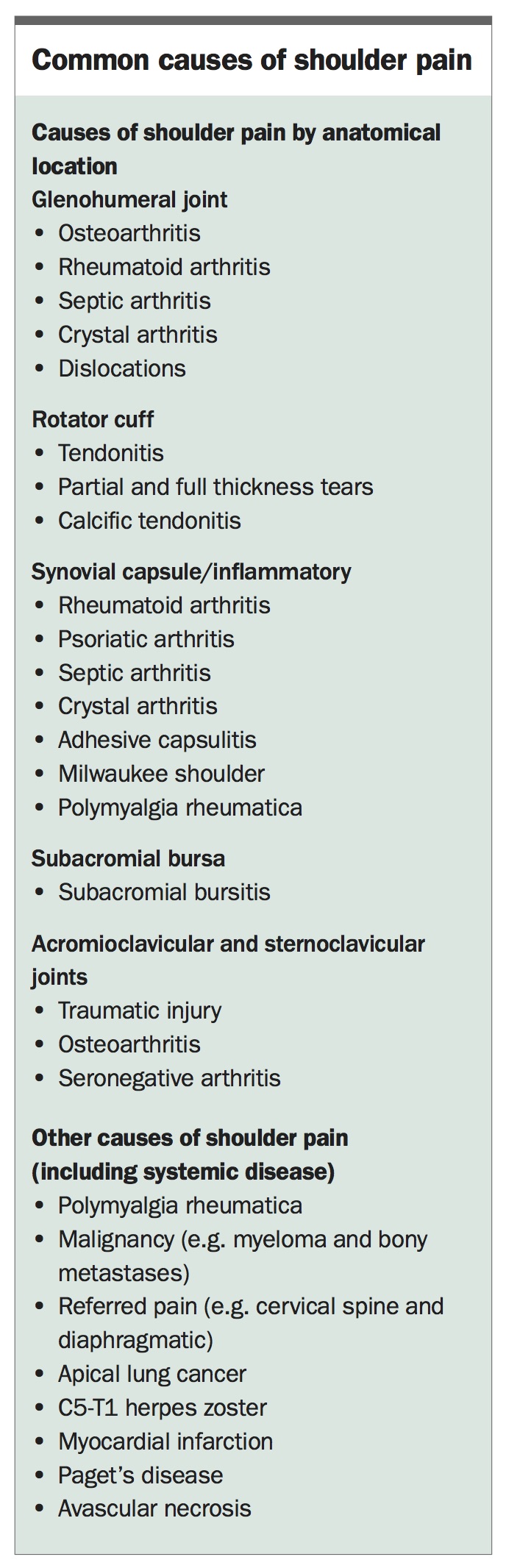
Abnormality in the shoulder can arise from each of these structures, with disorders of the rotator cuff being the most common cause of shoulder pain in primary care (Box).6
{kind=link}
Assessment of shoulder pain
Clinical assessment remains the cornerstone in formulating a working diagnosis when faced with the problem of a patient with shoulder pain. A thorough history should include an assessment of the onset and duration of pain, risk factors for shoulder pain (e.g. a history of trauma and certain occupations) and exclusion of extrinsic causes for pain and constitutional symptoms.7,8 Referred pain from the neck should always be considered in the medical assessment. This assessment should take into consideration red flag symptoms that may suggest serious underlying pathology, including malignancy, fracture, infection or visceral disease.
Confusion in the assessment of shoulder pain is compounded by inconsistent definitions for terms used to describe physical findings.9 A short glossary of commonly used terms when discussing shoulder pain is outlined below.
- Impingement or shoulder impingement syndrome. This term refers to clinical findings of pain on elevation of the shoulder or sleeping on the affected side thought to be most likely due to compression of soft tissue structures surrounding the shoulder, including tendons or bursae.10 There are multiple potential causes of impingement including rotator cuff disease, subacromial bursitis and osteoarthritis with the presence of osteophytes.
- Rotator cuff disease. This is an umbrella term encompassing symptomatic disorders of the rotator cuff muscles and related structures. It includes diagnoses such as rotator cuff tendinopathy, subacromial bursitis, rotator cuff tendon tears (full-thickness or partial thickness) and calcific tendonitis, but excludes adhesive capsulitis.9
- Adhesive capsulitis (frozen shoulder). This is a common shoulder complaint that is characterised by atraumatic onset of pain with progressive restriction of movement of the shoulder leading to functional impairment.11 Radiographic results suggest the pathology to be thickened glenohumeral joint capsule and synovium.12 This is more common in patients with diabetes mellitus, thyroid disorders and those with prolonged immobility such as following surgery or a stroke. Although commonly thought to resolve after two years, at a mean follow up of 4.4 years, 41% of patients still had ongoing symptoms.13
- Subacromial bursitis. This is inflammation of the subacromial bursa that may be provoked by trauma, prolonged pressure, overuse, crystal arthopathy or inflammatory arthritis such as rheumatoid arthritis or infection (septic bursitis). Subacromial bursitis may be acute or chronic and is often found to be present asymptomatically on imaging.1
There are a multitude of examination tests for patients with shoulder pain, some of which are described below.
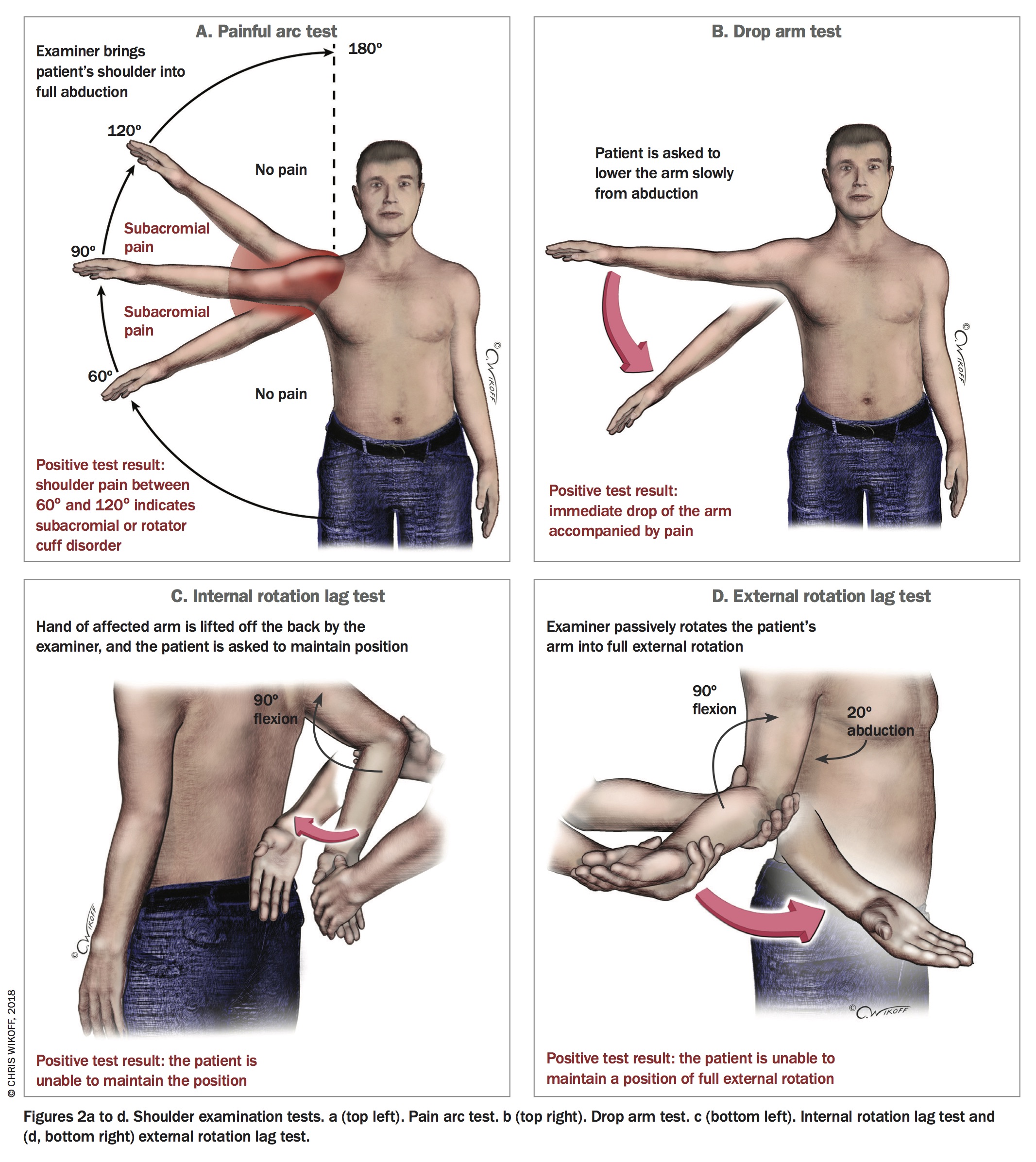
- Painful arc test. Provocation of pain on abduction of the shoulder between approximately 60 and 120 degrees indicates a positive painful arc test and may be associated with rotator cuff disease. Pain beyond 120 degrees suggests degeneration of the acromioclavicular joint (Figure 2a).14
- Drop arm test. The patient is asked to slowly lower the arm from 90 degrees abduction. An abrupt drop in the arm with pain indicates a positive test. If positive, this has a likelihood ratio of 3.3 for the presence of rotator cuff disease, indicating a moderate increase in the likelihood of disease (Figure 2b).15
- Hawkins test. This is a pain provocation test to elicit signs suggestive of shoulder impingement. With the patient’s elbow flexed to 90 degrees and held at 90 degrees flexion, the examiner internally rotates the shoulder.15
- Empty can test. In this test the patient holds the affected arm at 90 degrees abduction with 30 degrees adduction in the horizontal plane (or 30 degrees forward from the body) with the elbow extended, the forearm internally rotated and the thumb pointing down. The examiner exerts downward pressure proximal to the elbow and reproduction of weakness or pain indicates a positive test and suggests the presence of rotator cuff disease.15
- Internal and external rotation lag tests. The examiner moves the shoulder through passive internal and external rotation with the elbow flexed to 90 degrees. Internal rotation is assessed with the patient’s hand behind their back and the hand lifted away from the back. It can be documented by noting the level of the dorsal spine reached with the thumb (Figure 2c). External rotation is assessed with the shoulder at 20 degrees abduction and inability to maintain the shoulder in external rotation suggests a full tear of a rotator cuff usually involving supraspinatus, infraspinatus and teres minor (Figure 2d).15
{kind=link}
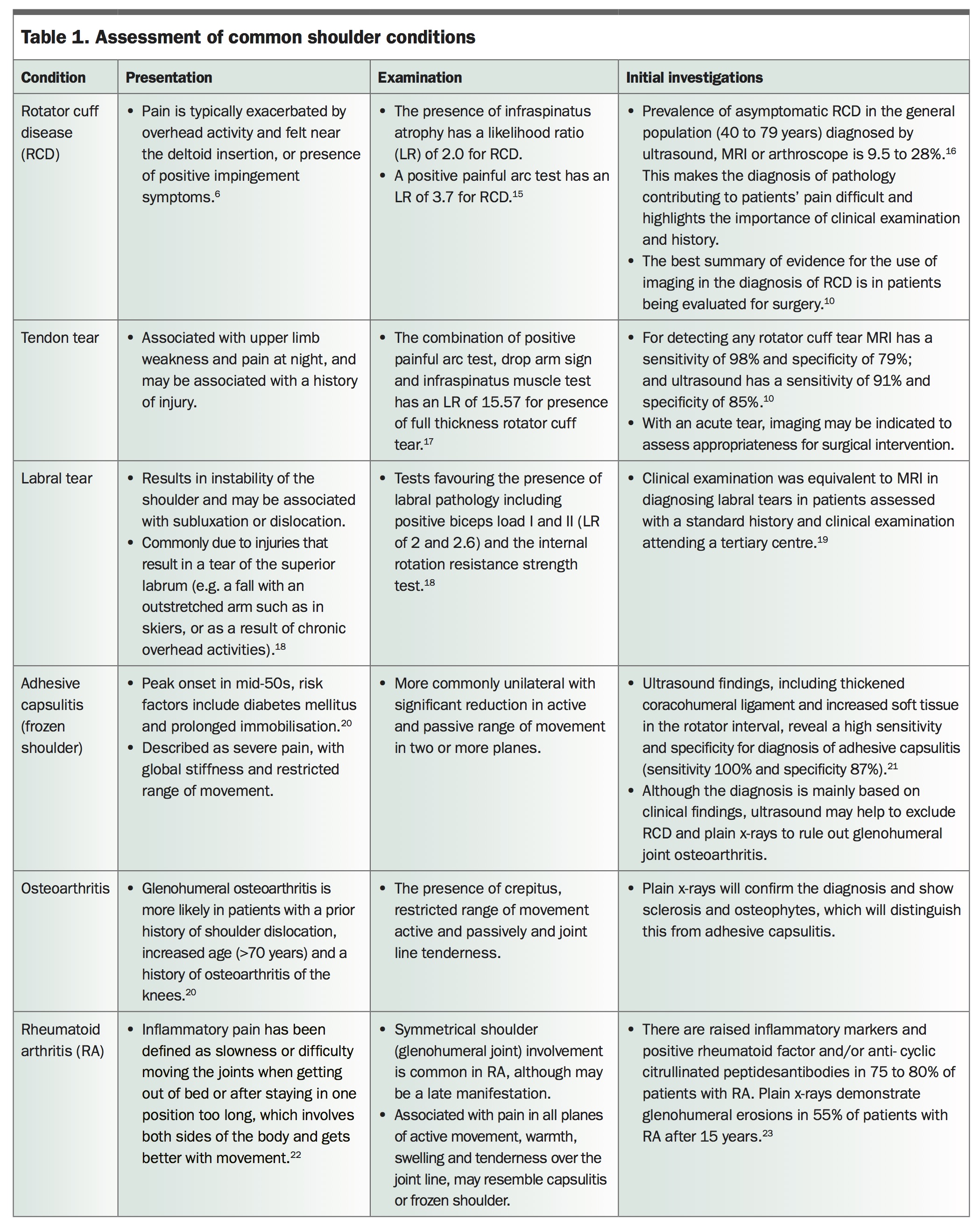
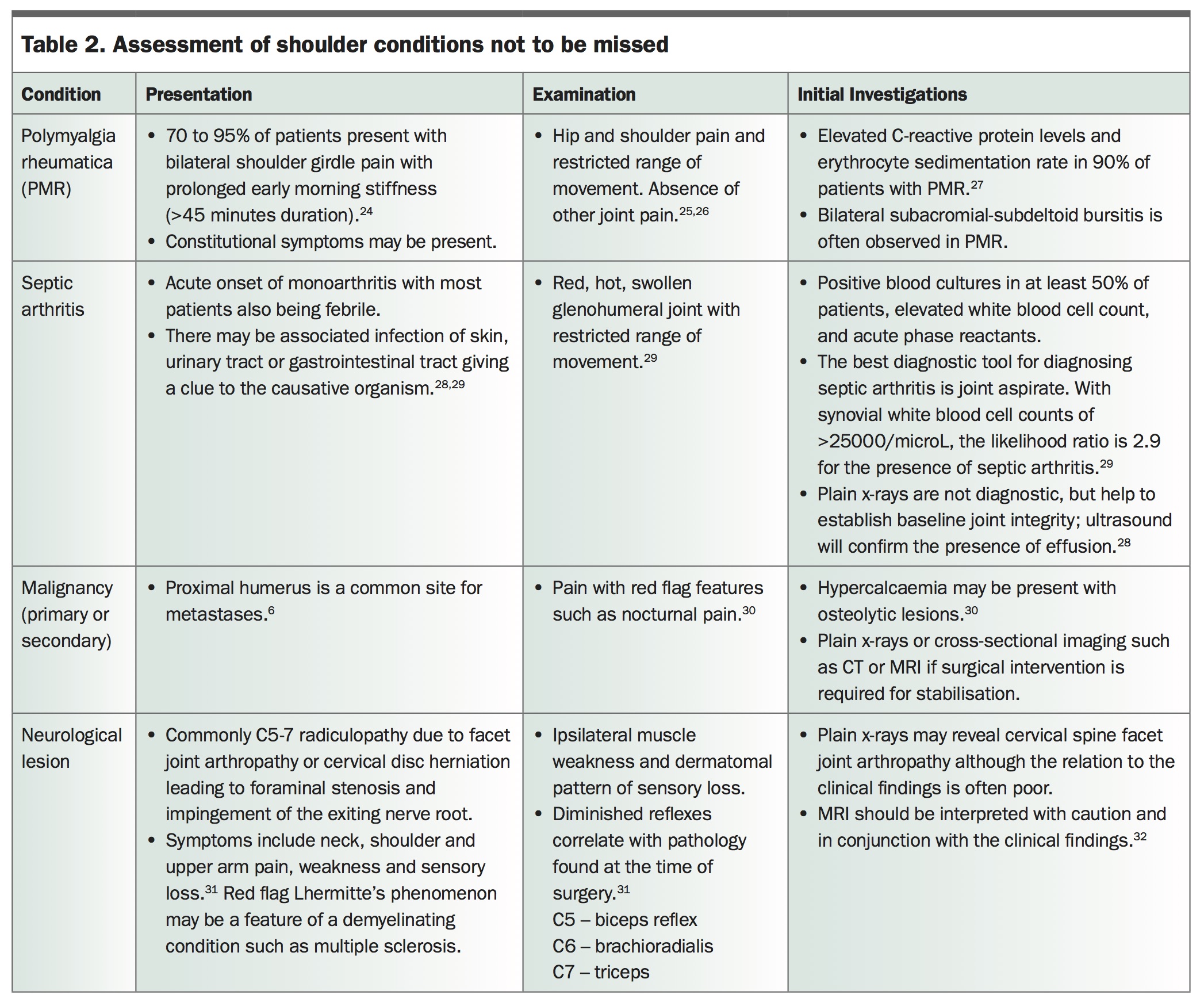
Clinical examination remains an important part of the investigation for causes of shoulder pain. A complete yet concise clinical examination of the shoulder has been developed by Battistone and Baker at the Veterans Affairs Medical Centre in Salt Lake City, Utah (available online at www.youtube.com/watch?v=dzHFwkXBmvU). The clinical features and suggested investigations for common shoulder pain presentations and shoulder presentations not to be missed are outlined in Table 1 and Table 2.6,10,15-32
{kind=link}
{kind=link}
There are two basic types of examination manoeuvres in the assessment of shoulder complaints, namely movement-based pain provocation tests and strength tests. In regard to pain provocation tests, the painful arc test, rather than the Hawkins test, is more likely to demonstrate the presence of rotator cuff disease. Of the strength tests, the external and internal rotation lag tests if positive are most likely to demonstrate the presence of rotator cuff tears.15
Commonly employed imaging for the investigation of shoulder pain includes plain x-rays, ultrasound and magnetic resonance imaging. Although, there are no current guidelines internationally or nationally to recommend a diagnostic approach for the investigation of shoulder pain, investigations are advised for patients with atypical or concerning clinical features to exclude pathology such as fracture, dislocation or lytic lesions, or in whom intervention is being considered.6,7 Unfortunately many of the radiological investigations for shoulder pain often have frequent false positives, due to the high of asymptomatic shoulder disease. This was demonstrated in a community-based study of 664 residents which found that 22% of the population had a rotator cuff tear on ultrasound of bilateral shoulders, with asymptomatic rotator cuff tears accounting for 65.3% of all tears, and symptomatic tears accounting for 34.7%.33
Plain x-rays remain the initial radiographical investigation of choice in most cases. Plain x-rays identify osteoarthritis and erosive changes suggestive of inflammatory arthritis or Milwaukee shoulder, and exclude lytic or sclerotic lesions. They should be performed if shoulder pain is persistent or if considering an invasive intervention. A recent systematic review comparing ultrasound with magnetic resonance imaging in the detection of rotator cuff tears found them to be comparable, and so it is reasonable to consider local availability and surgeon preference when considering between these two modalities.10
When to refer
A trial of noninvasive therapies such as simple analgesia and/or NSAIDs may well be appropriate for patients with shoulder pain before any referral. Patients likely to respond best to a conservative approach include those with an intact intramuscular tendon of supraspinatus, minimal atrophy of the supraspinatus tendon, negative impingement signs and preserved motion in external rotation.
Many patients with rotator cuff disease or adhesive capsulitis will probably receive improvements in overall pain and function with manual therapy and exercise.11,34 The Royal Australian College of General Practitioners is in the process of updating the practice guidelines for the management of osteoarthritis.
Patients should be offered referral to secondary care in the presence of any concerning or red flag features such as nocturnal pain, trauma, constitutional symptoms or raised inflammatory markers or if there is a prolonged duration of symptoms with diagnostic uncertainty.7 Surgeons specialise in the management of structural pathology, for example, severe glenohumeral osteoarthritis or degeneration and tendon tears, although the evidence base for several surgical interventions is limited.35 Features that may trigger referral of the patient to an orthopaedic surgeon include shoulder pain that is particularly disabling (e.g. in an athlete or a labourer) or a history of trauma or recurrent joint instability or weakness.7
In the absence of an indication for surgical intervention, other options include referral of the patient to a rheumatologist (particularly if inflammatory disease is suspected) or an occupational physician in the case of work-related shoulder pain. Other sources of help may include rehabilitation physicians or practitioners with a special interest in musculoskeletal medicine.
Occupational and sporting activities are risk factors for rotator cuff disease. In situations where the problem is slow to improve it is appropriate to consider a biopsychosocial approach to managing the pain.8 This approach may also involve seeking assistance from a range of practitioners including psychologists and pain management specialists.
Depending on the cause of the patient’s shoulder pain and the nature of the management that is required, the patient should be referred back to the GP for ongoing care, co-ordination and regular assessment following the initial assessment and management.
Conclusion
The clinical assessment, including a targeted history and examination, remains the most important part of the diagnostic process for patients presenting with shoulder pain. An examination that includes a painful arc test and an assessment of shoulder strength including the internal and external lag tests will provide clinicians with helpful clues to the underlying pathology. Subsequent investigation and treatment should be guided by the initial clinical findings and tailored to the progress of the patient’s symptoms. Referral of the patient for specialist advice is recommended for specific situations, such as the need for surgery or the presence of red flags or refractory symptoms. PMT
References
9: 272-280.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.